In order to minimize the possibility of postoperative nerve adhesion, it is necessary to always pay attention to the principle of preventing adhesion during sacral cyst surgery.
With regard to adhesions, it is imperative to emphasize several key concepts: Firstly, adhesions can occur in any surgical procedure, and it is impossible to completely avoid postoperative adhesions. Secondly, a certain level of adhesion is crucial for effective treatment. For instance, during the repair of a sacral cyst leak, some degree of adhesion is necessary to ensure a complete seal and prevent recurrence. Similarly, the suturing of an incision necessitates adhesion between tissues on both sides to prevent the incision from cracking after suture removal, particularly in malnourished patients. Therefore, necessary adhesion is essential for achieving therapeutic outcomes. Thirdly, a minimal amount of adhesion typically does not cause discomfort or symptoms. This is evident in neurosurgical procedures such as trigeminal neuralgia, hemifacial spasm surgery, lumbar disc herniation surgery, and acoustic neuroma surgery, where direct surgery on the nerves is involved. Postoperatively, a small amount of adhesion around the nerves is inevitable but usually painless and asymptomatic. The same applies to sacral cyst surgery. Lastly, the primary focus should be on preventing and overcoming “excessive adhesion,” particularly when a significant number of scars tightly envelop multiple nerve roots or when scars inside and outside the spinal canal become adhered.
Dr. Zheng shared a typical case to illustrate how to implement the concept of sacral cyst anti-adhesion surgery.
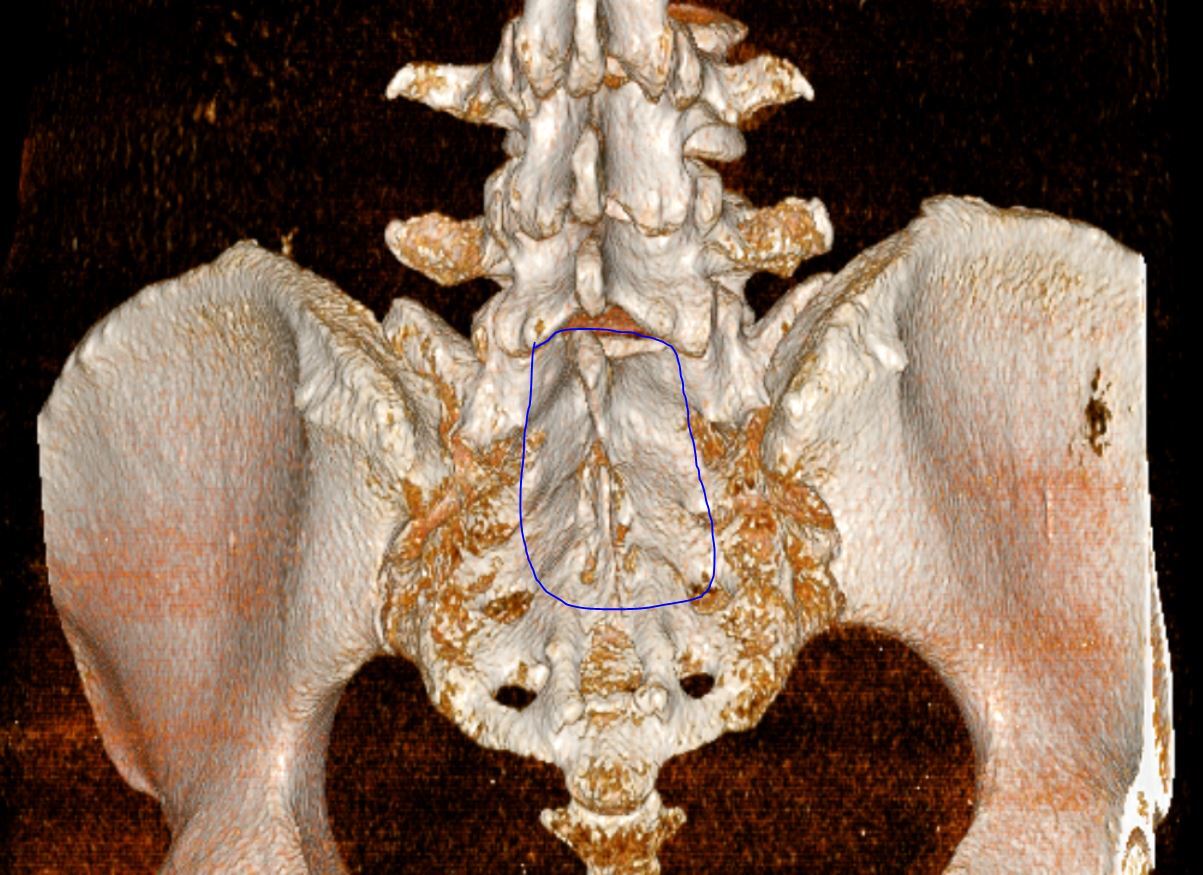
The patient presents with a 3.5cm sacral cyst. The conventional surgical technique for this type of cyst involves making an incision along the blue line to expose the entire sacral canal, thereby accessing the sacral lumen. Following the surgical procedure, the posterior wall of the sacral canal is restored using titanium connectors and screws.
The patient has a single, large sacral cyst, with the leak affecting only one nerve root, regardless of its size. Utilizing the conventional surgical method would result in the exposure of all sacral nerve roots. Subsequently, any exposed nerve roots would develop adhesions postoperatively, inevitably leading to “excessive adhesions.”
The concept of sacral cyst anti-adhesion surgery differs in several key aspects:
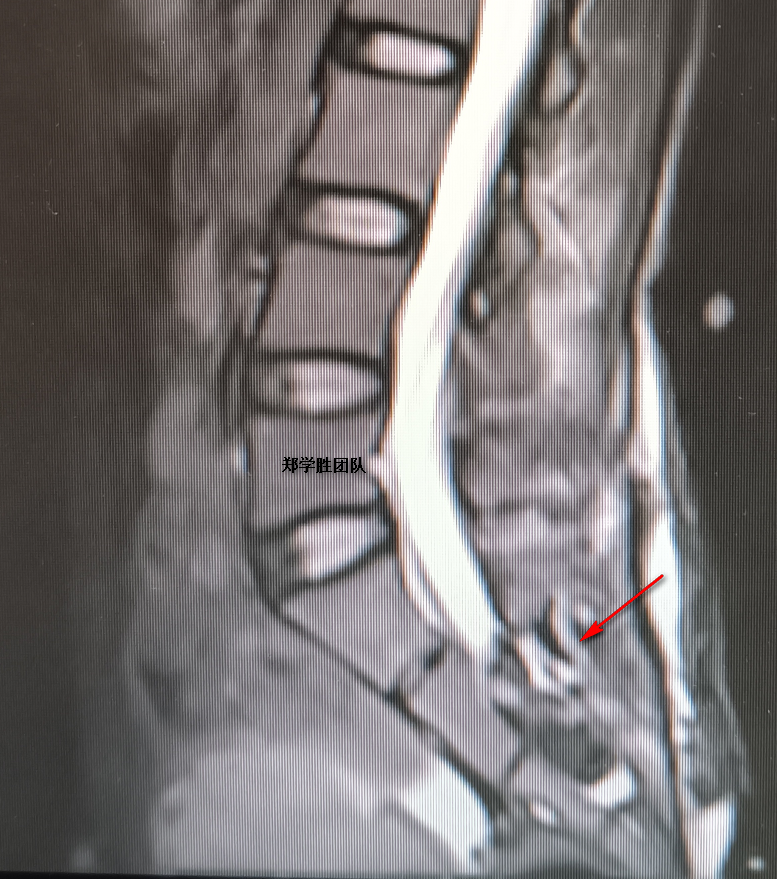
1. Preoperative imaging is utilized to accurately locate the sacral cyst leakage.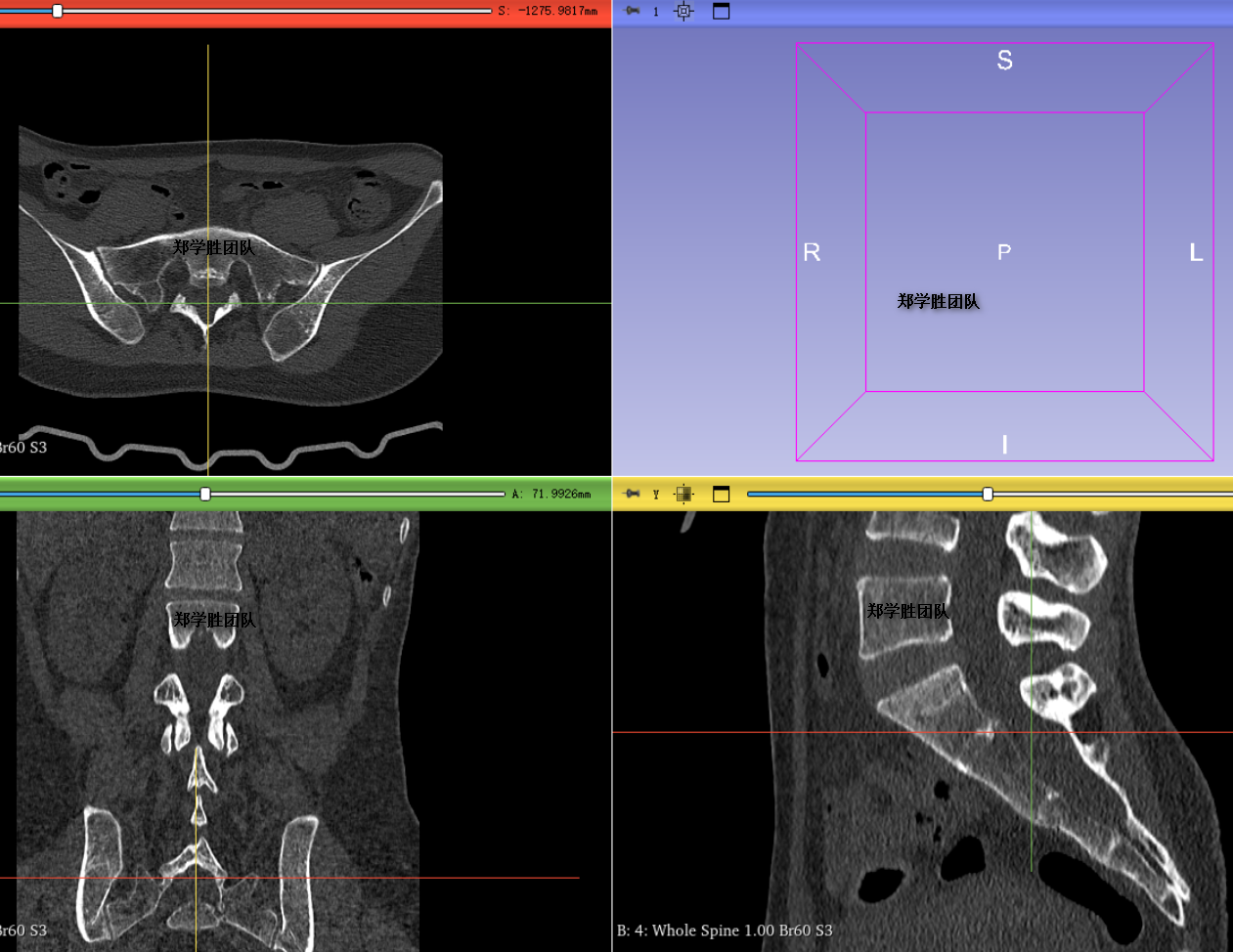
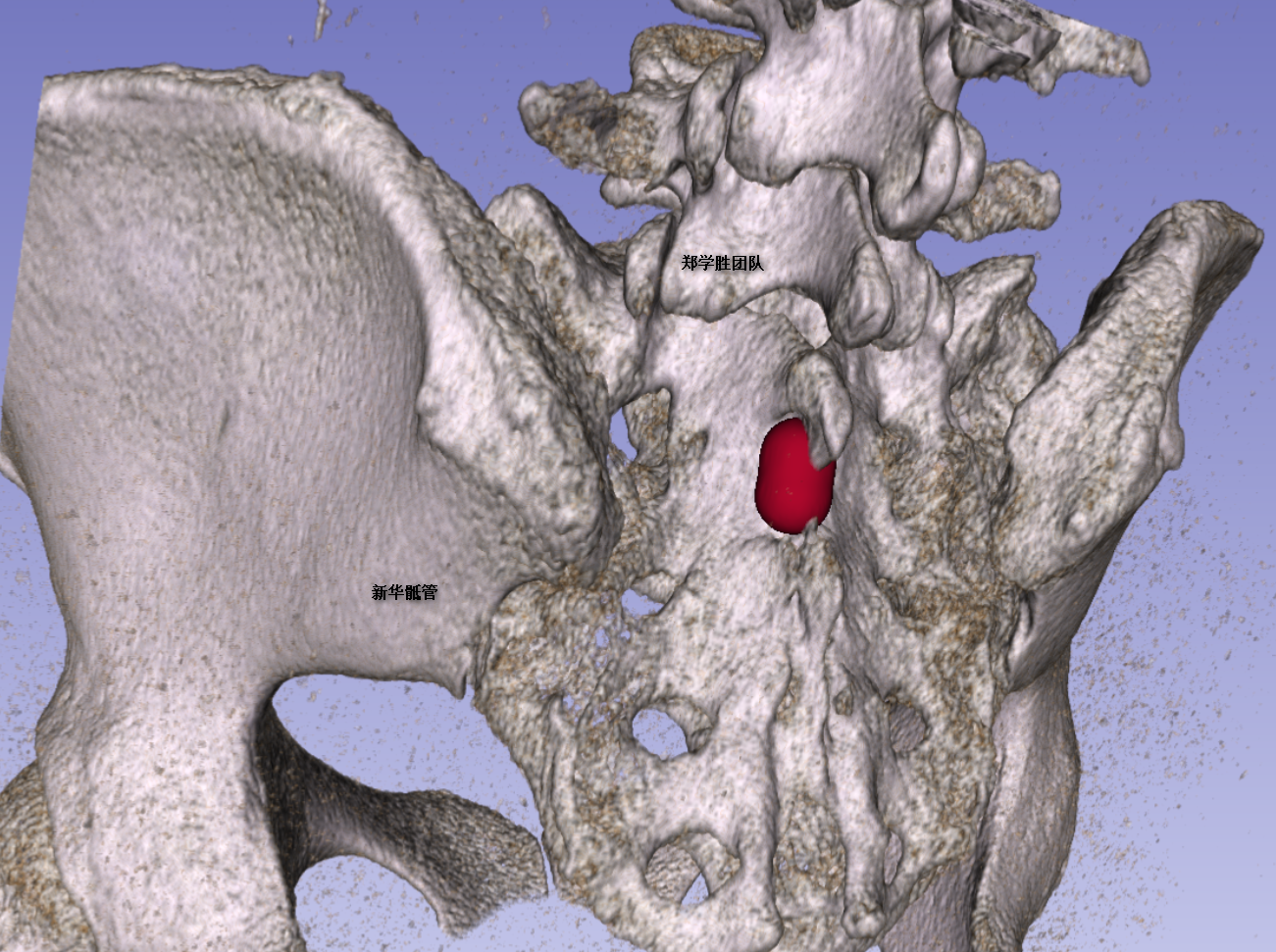
2. During the surgery, a small bone window is created at the weakest point of the posterior wall of the sacral canal, facing the location of the leakage, based on the leakage’s position.
3. Through this tiny bone window, only the nerve root affected by the leak is exposed. The leak is then microscopically sutured and sealed, ensuring that the other nine nerve roots remain unexposed and unaffected.
4. At the conclusion of the surgery, a small titanium plate is used to repair the bone window, preventing adhesion between the inside and outside of the spinal canal. Postoperative CT reconstruction confirms that the position and size of the bone window align with preoperative planning.