Posted
Author Xuesheng Zheng
Posted
A 25-year-old male patient was admitted to the hospital due to a growing mass in the lower right abdomen for two months, accompanied by stool weakness and constipation. Additionally, he experienced soreness and pain in the lumbosacral region, rendering him unable to stand or sit for prolonged periods and hindering his ability to maintain work performance.
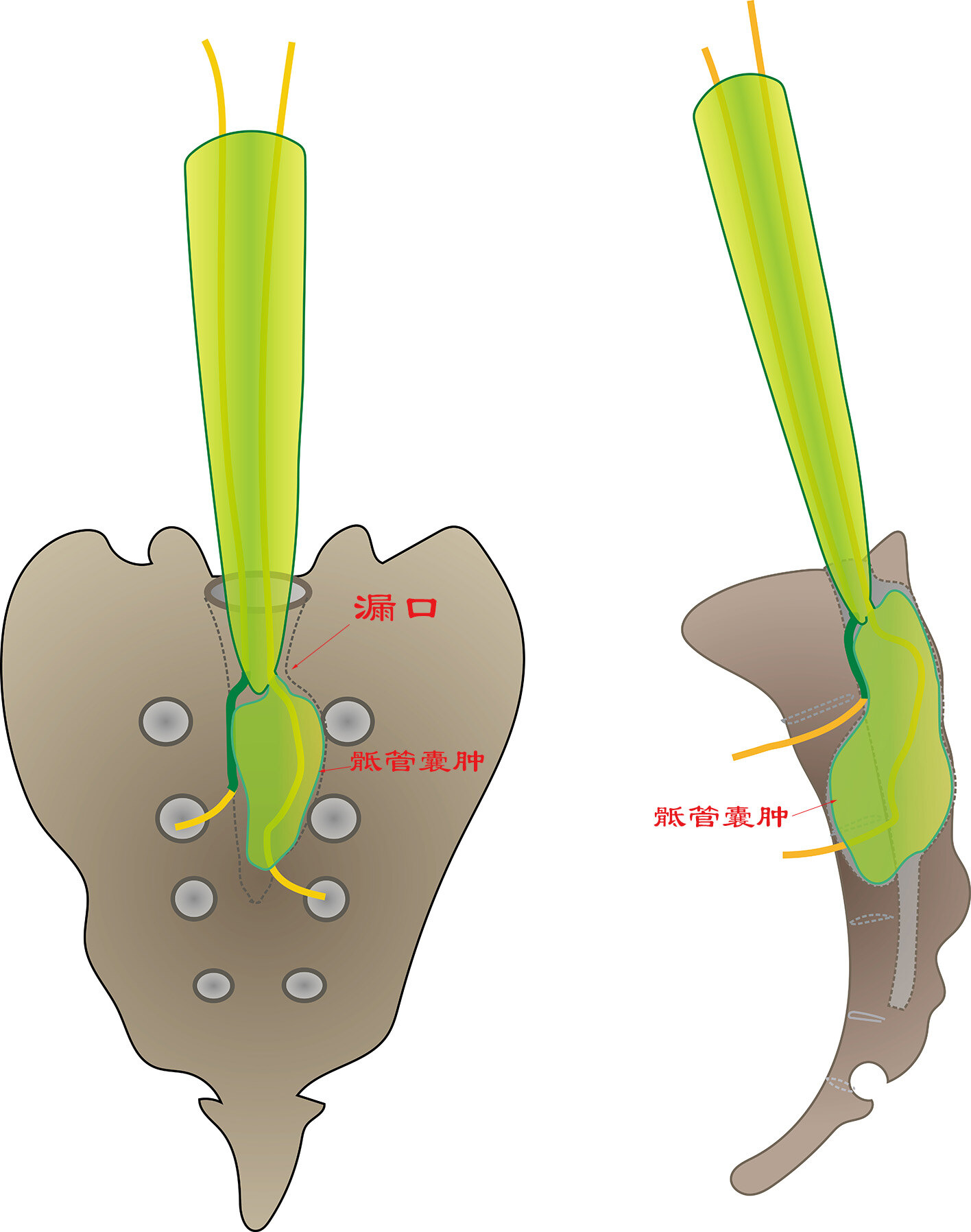
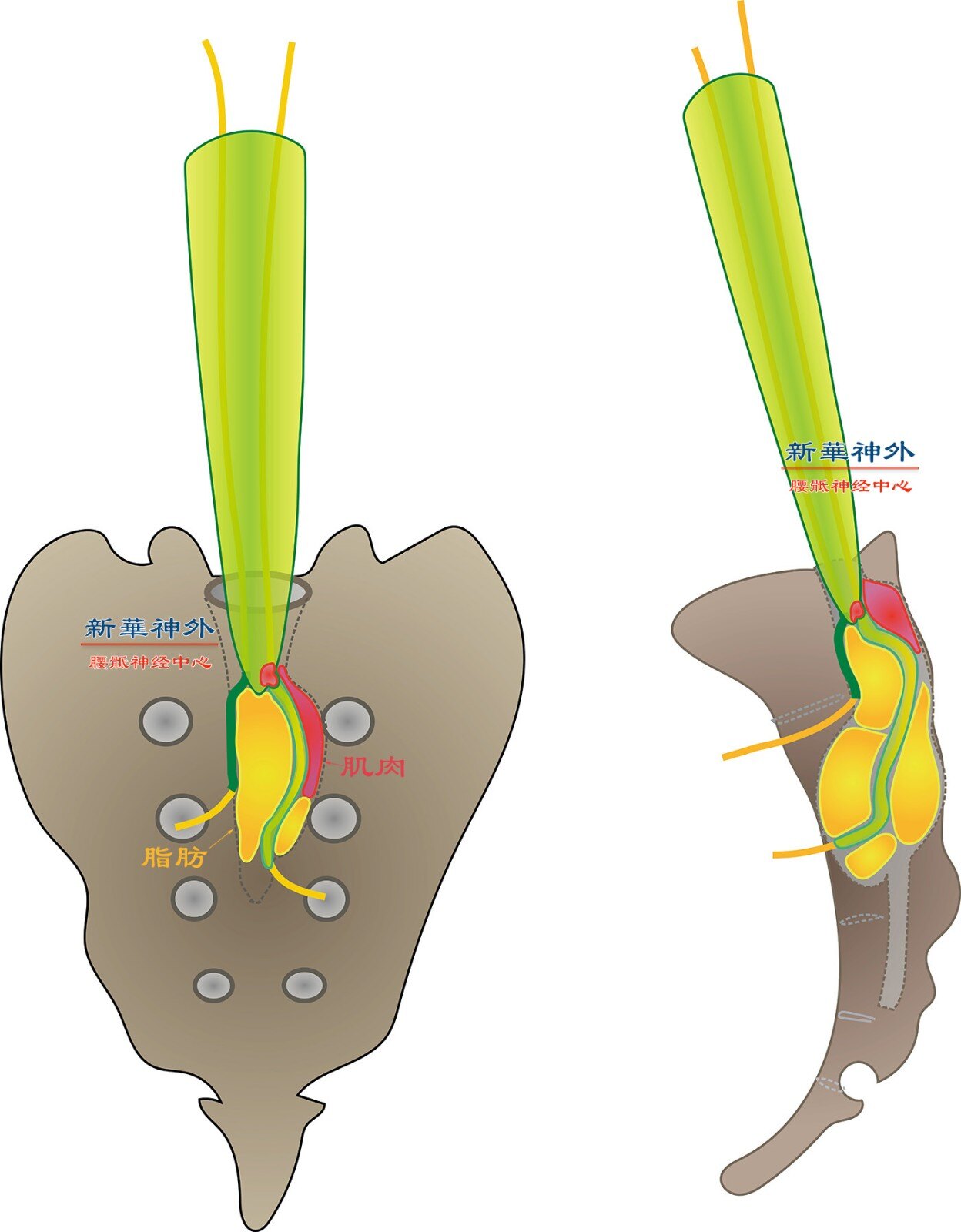
Magnetic resonance imaging revealed a huge sacral cyst that had protruded through the sacral foramen into the pelvic cavity, forming a spherical cystic mass exceeding ten centimeters in size. Furthermore, the cyst had penetrated the posterior wall of the sacral canal, creating a conical cystic mass within the intermuscular space.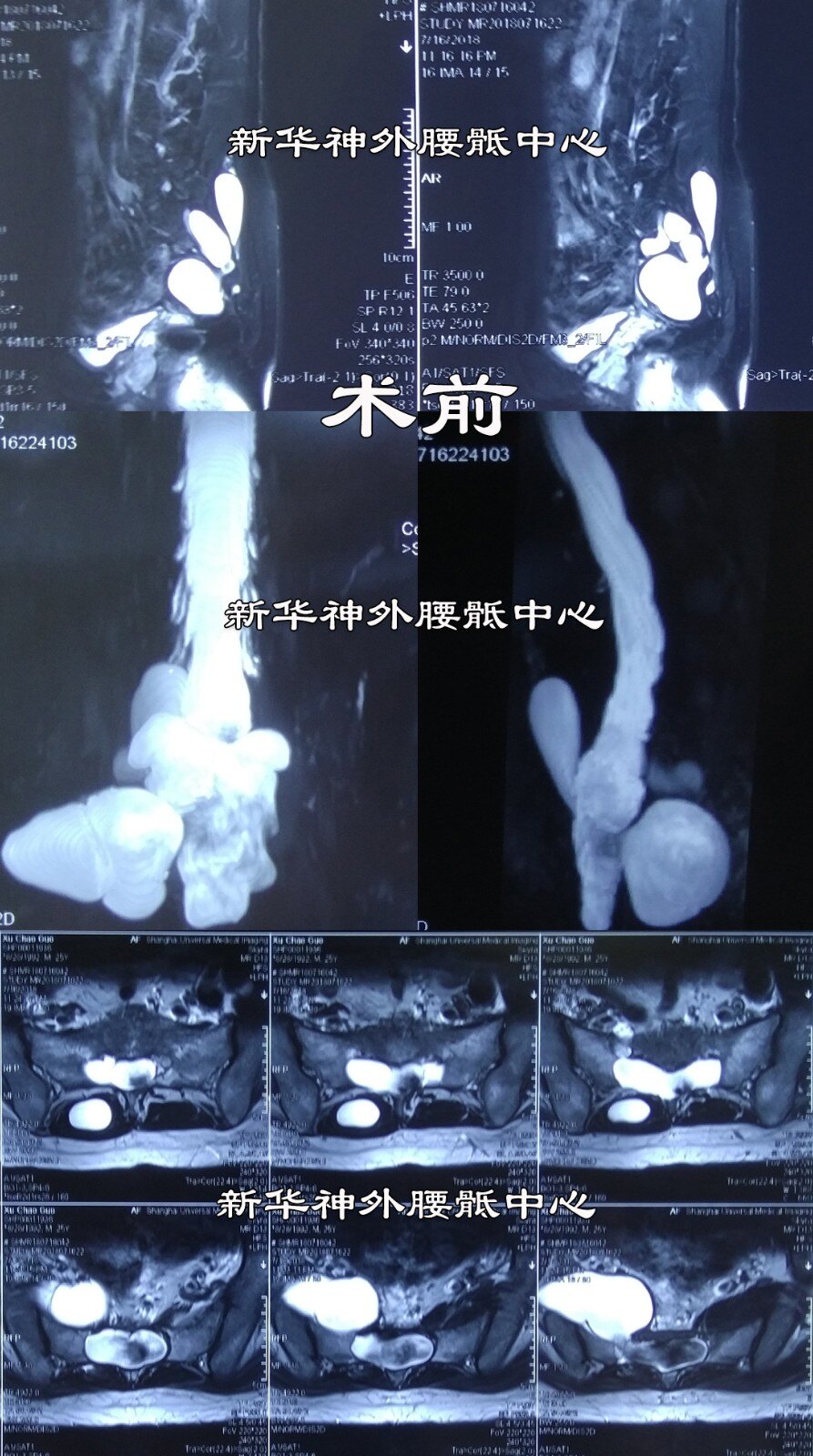
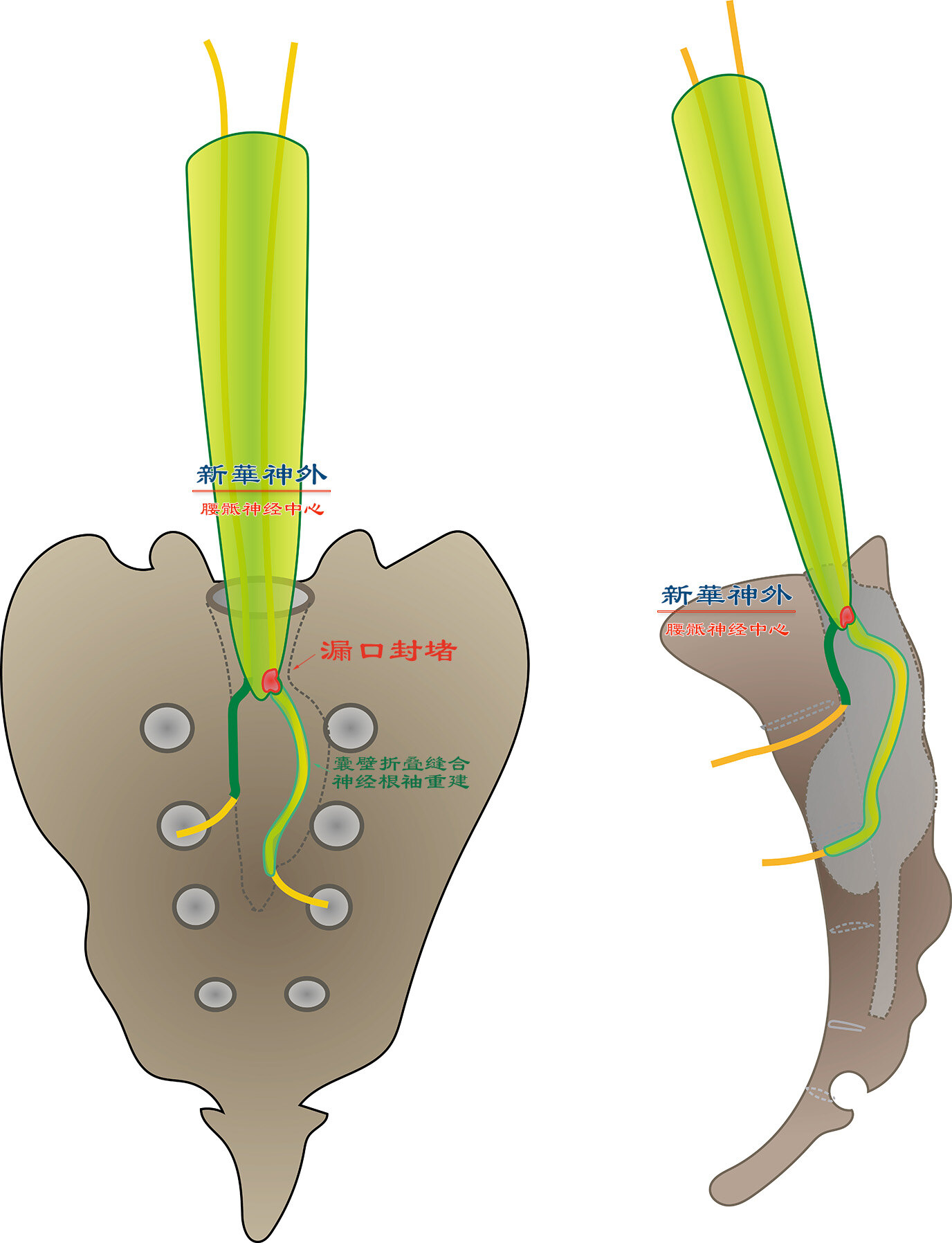
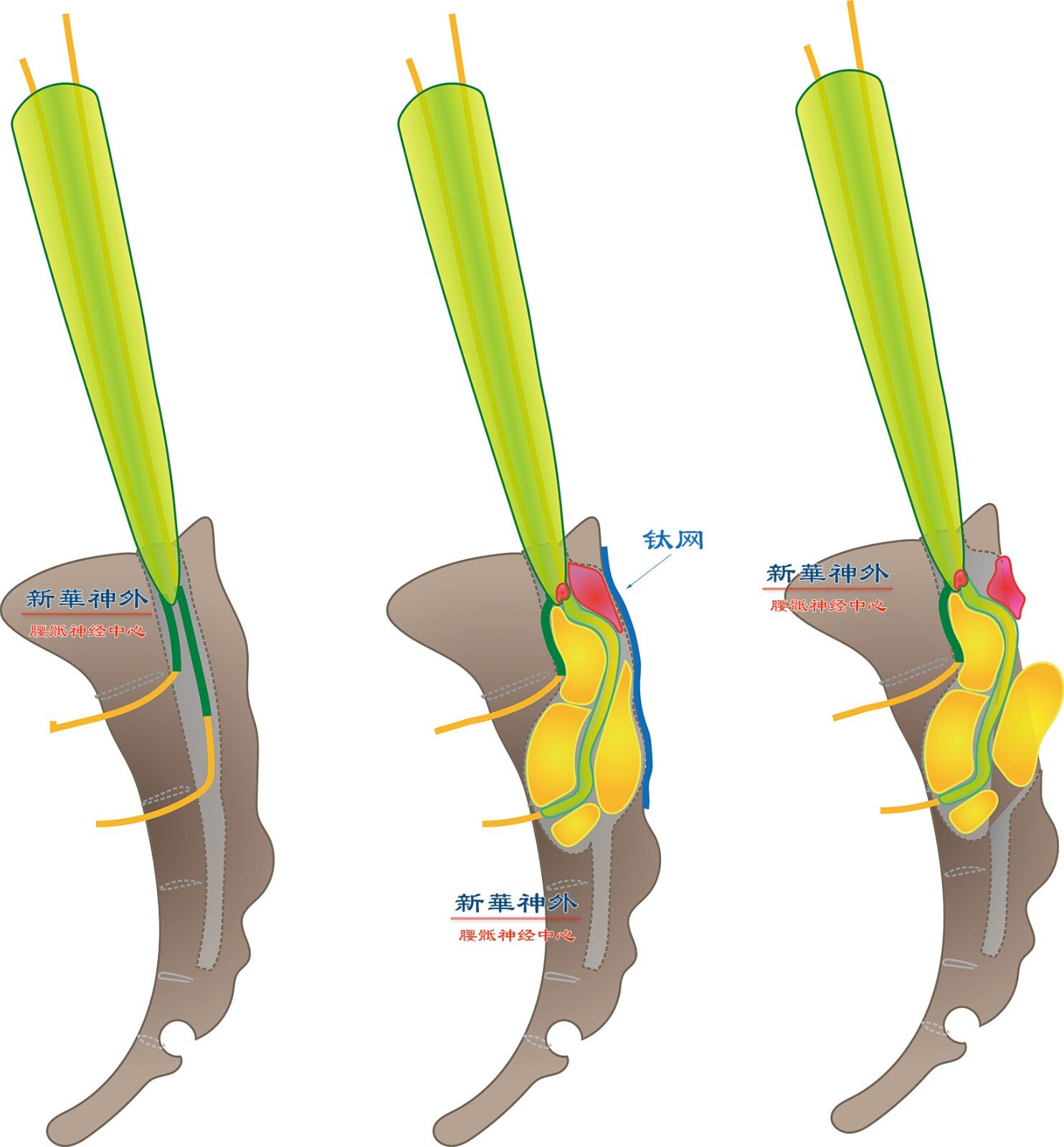
During surgery, it was discovered that the sacral cyst had a big leak, which was promptly sealed while ensuring the protection of transversing nerves.
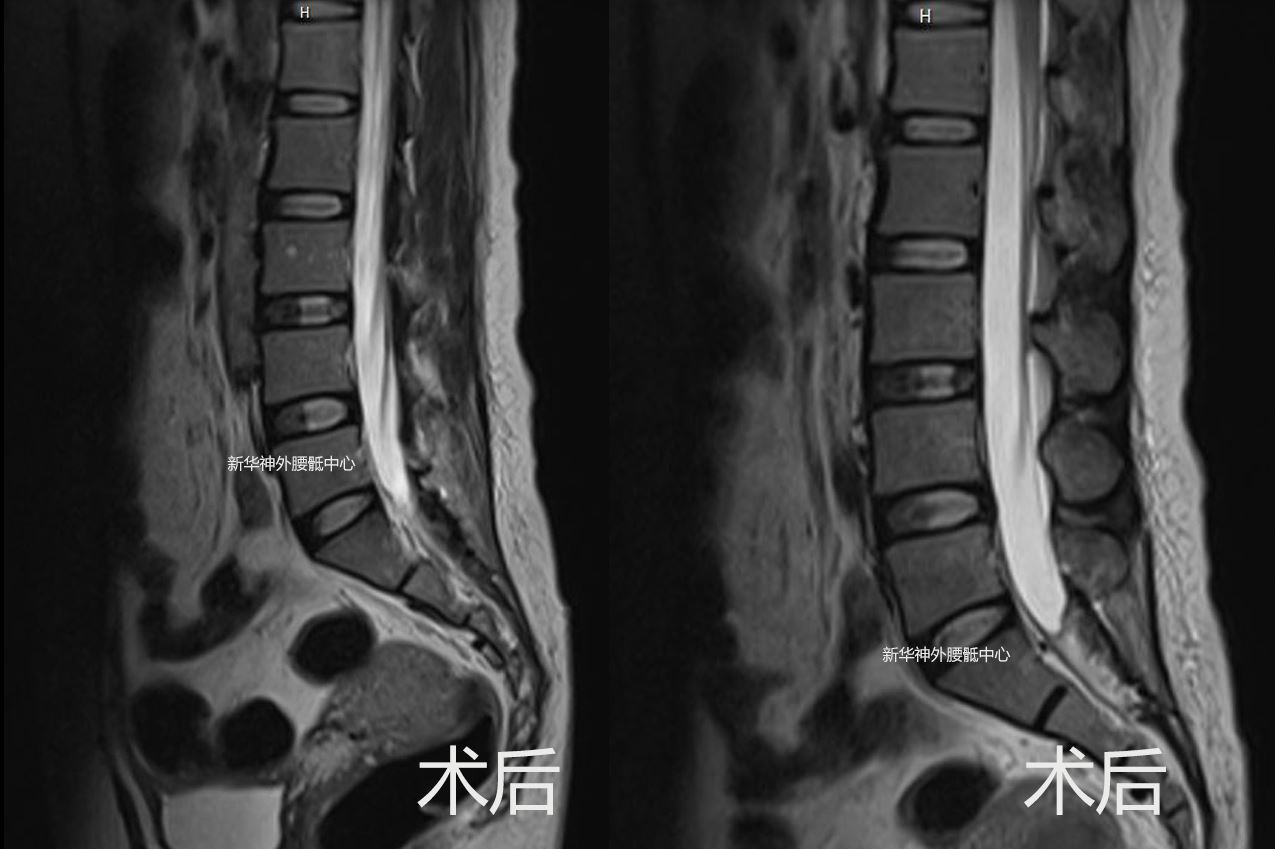
Follow-up magnetic resonance imaging conducted within one year post-surgery demonstrated successful occlusion of the cyst with no signs of recurrence. To date, the patient has been under follow-up care for nearly two years.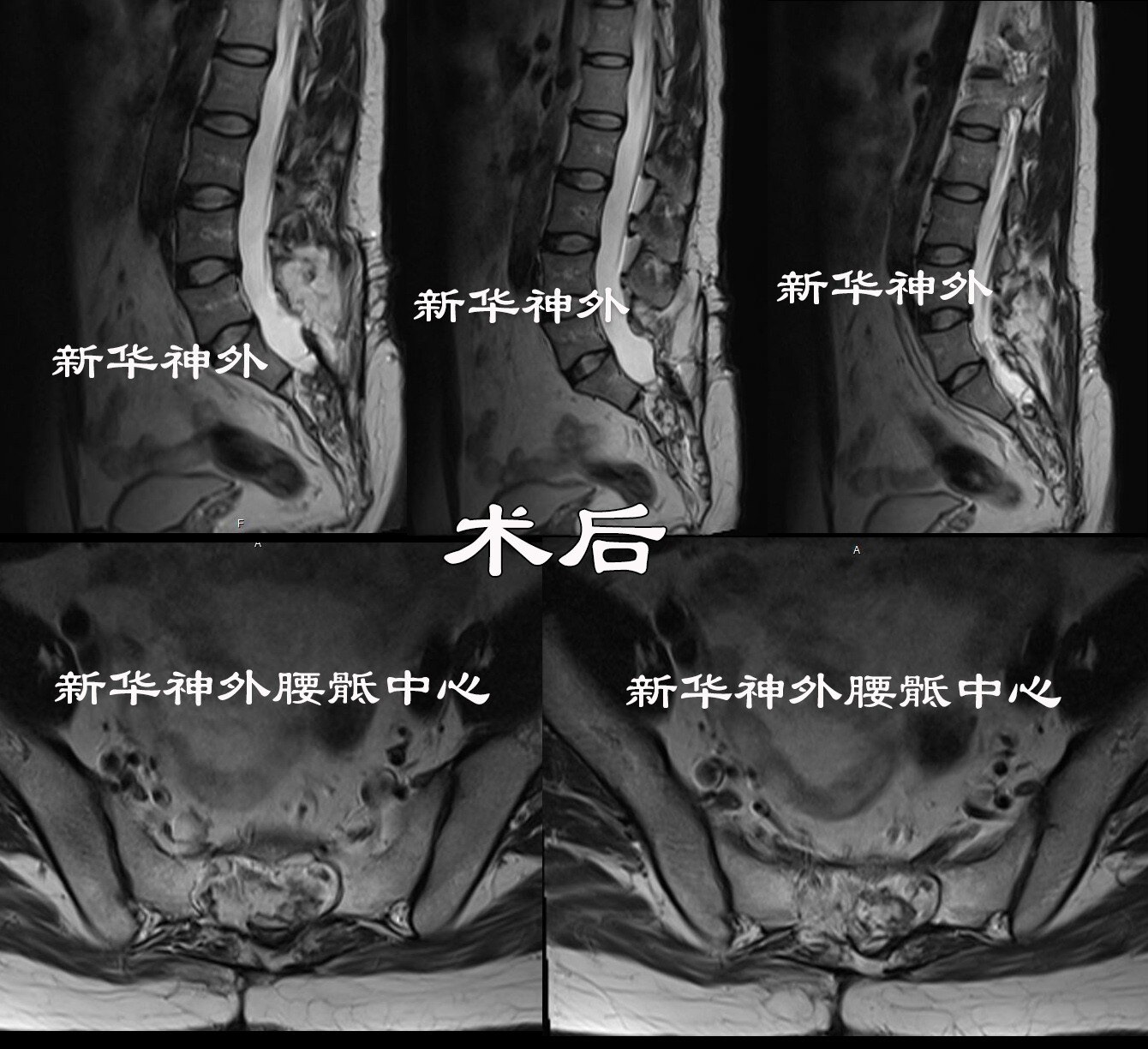
All symptoms subsided rapidly, and bowel movements recovered to normal. The patient resumed his work responsibilities three months after surgery.
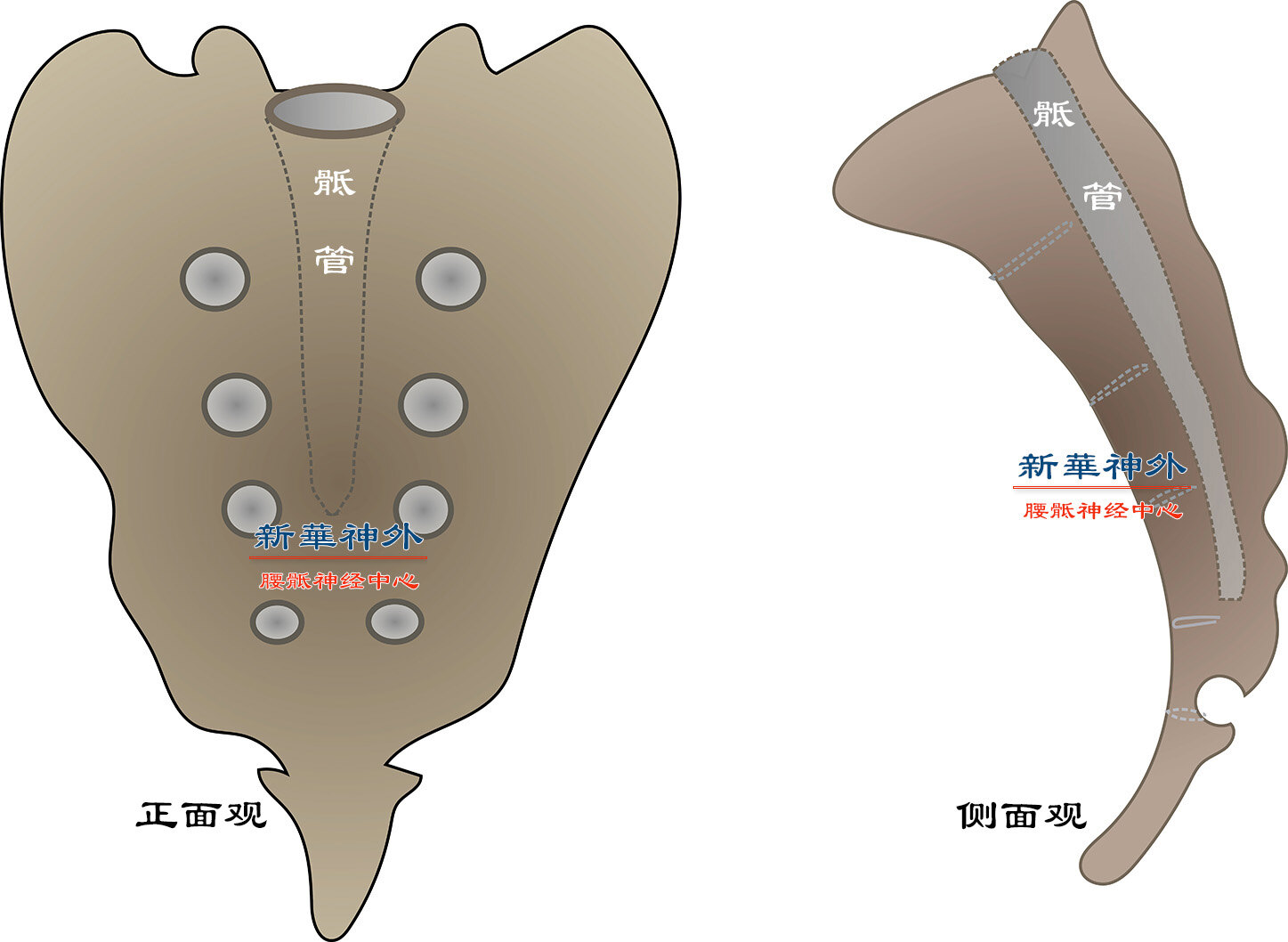
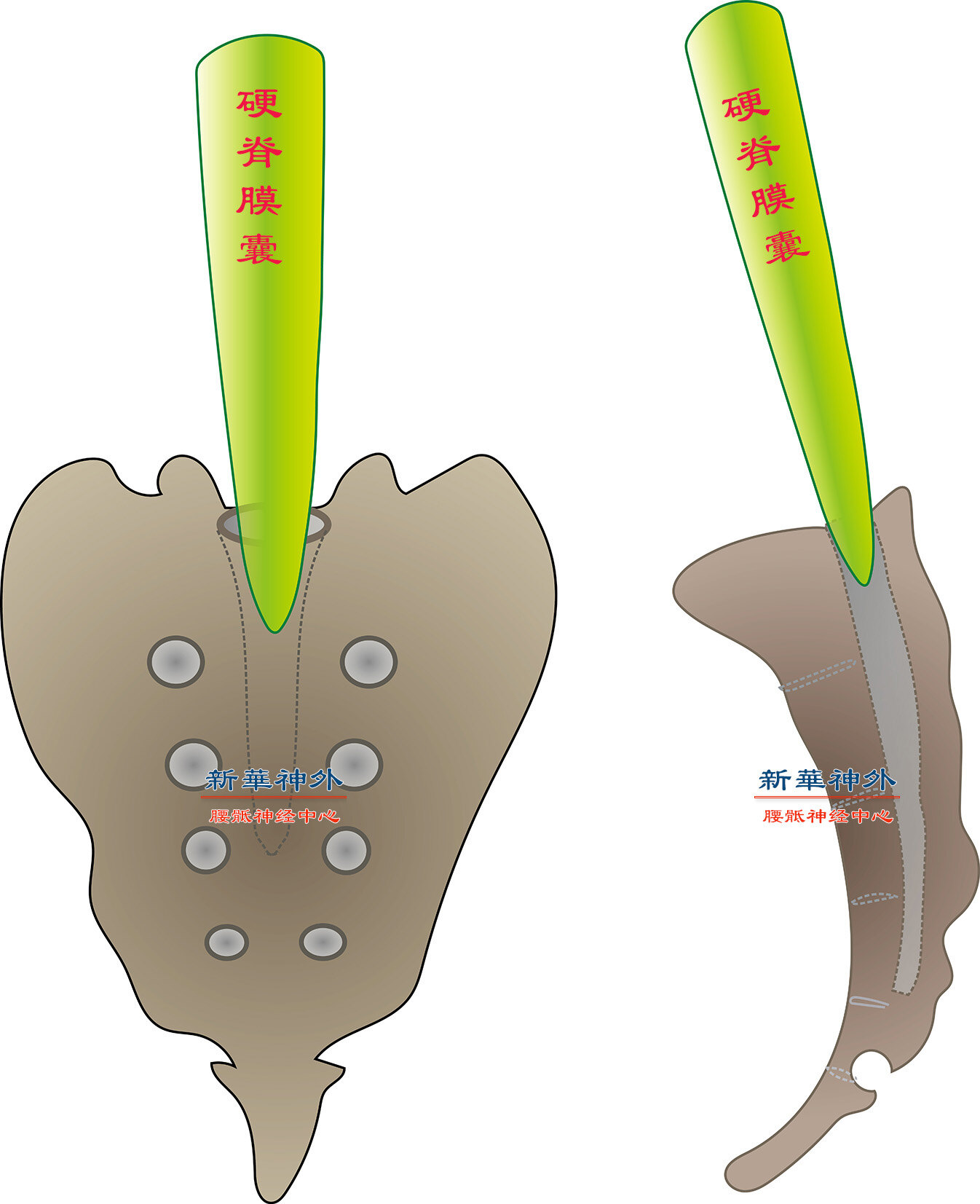
Dr. Zheng Xuesheng emphasized that the prolonged exposure of sacral cysts to substantial static water pressure can lead to damage to the sacral vertebral body, which typically has a thickness of 3-4 centimeters. This damage allows the cyst to protrude into the pelvic cavity. Once in the pelvic cavity, the cyst loses the bone restriction, enabling rapid enlargement. In this particular case, the cyst affected bowel function within two months, causing stool weakness and constipation. If left untreated, it was anticipated that urinary and sexual function would suffer irreversible damage in the near future. Fortunately, the patient underwent timely surgery, resulting in swift postoperative recovery. Given his youthful and robust constitution, he was able to resume his duties within three months.Author Xuesheng Zheng
Posted
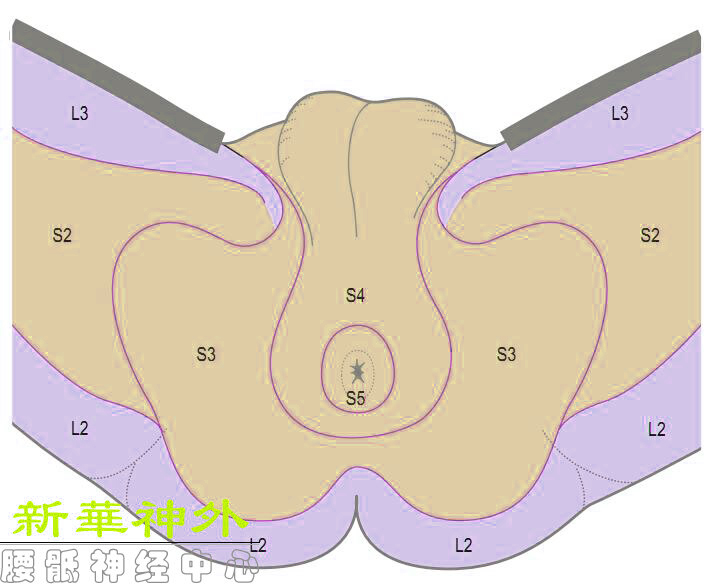
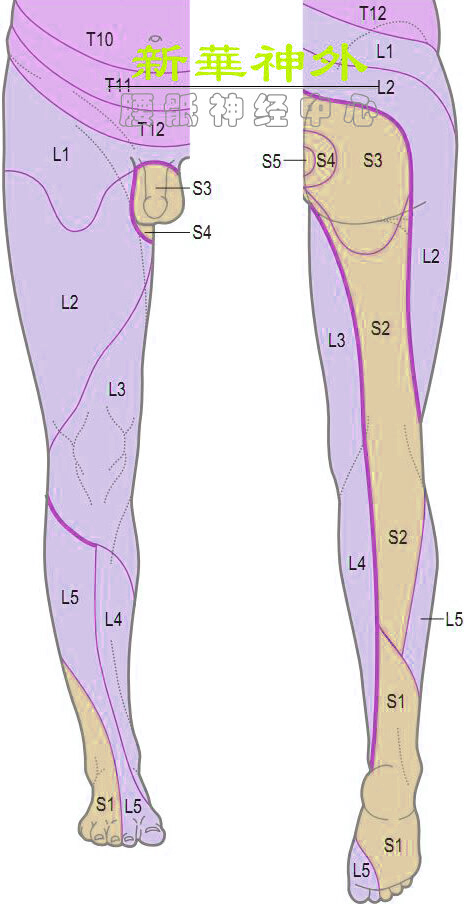
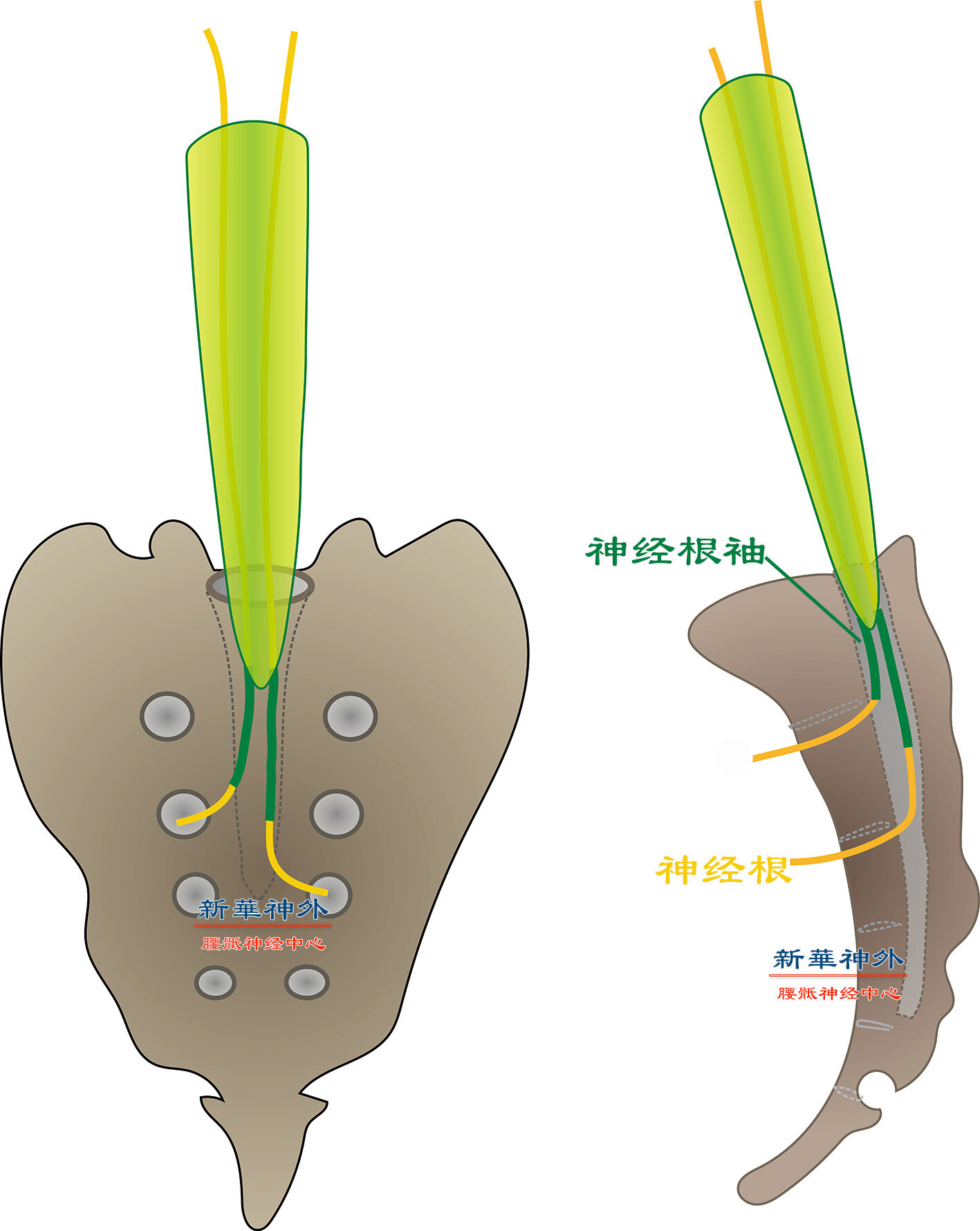
The first sacral nerve root (S1) is primarily responsible for skin sensation behind the calf, heel, and sole, while the second sacral nerve root (S2) covers the sensation behind the thigh, upper thigh, and posterior calf. The skin sensation of the buttocks, anus, and perineum is mainly innervated by the third, fourth, and fifth sacral nerve roots (S3, S4, S5).
Sacral cysts can compress nerve roots, leading to varying symptoms depending on the pressure. Typically, prolonged standing or sitting increases pressure and exacerbates pain, which improves upon resting in a supine position.
Large sacral cysts can compress nerve roots on both sides due to the limited width of the sacral canal (approximately 1.5cm). For instance, a cyst originating from the left side can affect the right-side nerve roots if sufficiently large. Similarly, cysts originating from upper nerve roots may compress both the corresponding and lower nerve roots, causing pain in various areas such as the heel, posterior calf, anus, and perineum. However, cysts from lower nerve roots typically do not affect upper nerve roots. These principles contribute to the wandering pain sites and fluctuating pain levels observed in sacral cysts.
It’s crucial to note that painful skin segment distribution varies significantly among individuals and should not be interpreted mechanically. Instead, it requires comprehensive evaluation alongside other neurological signs.Author Xuesheng Zheng
Posted
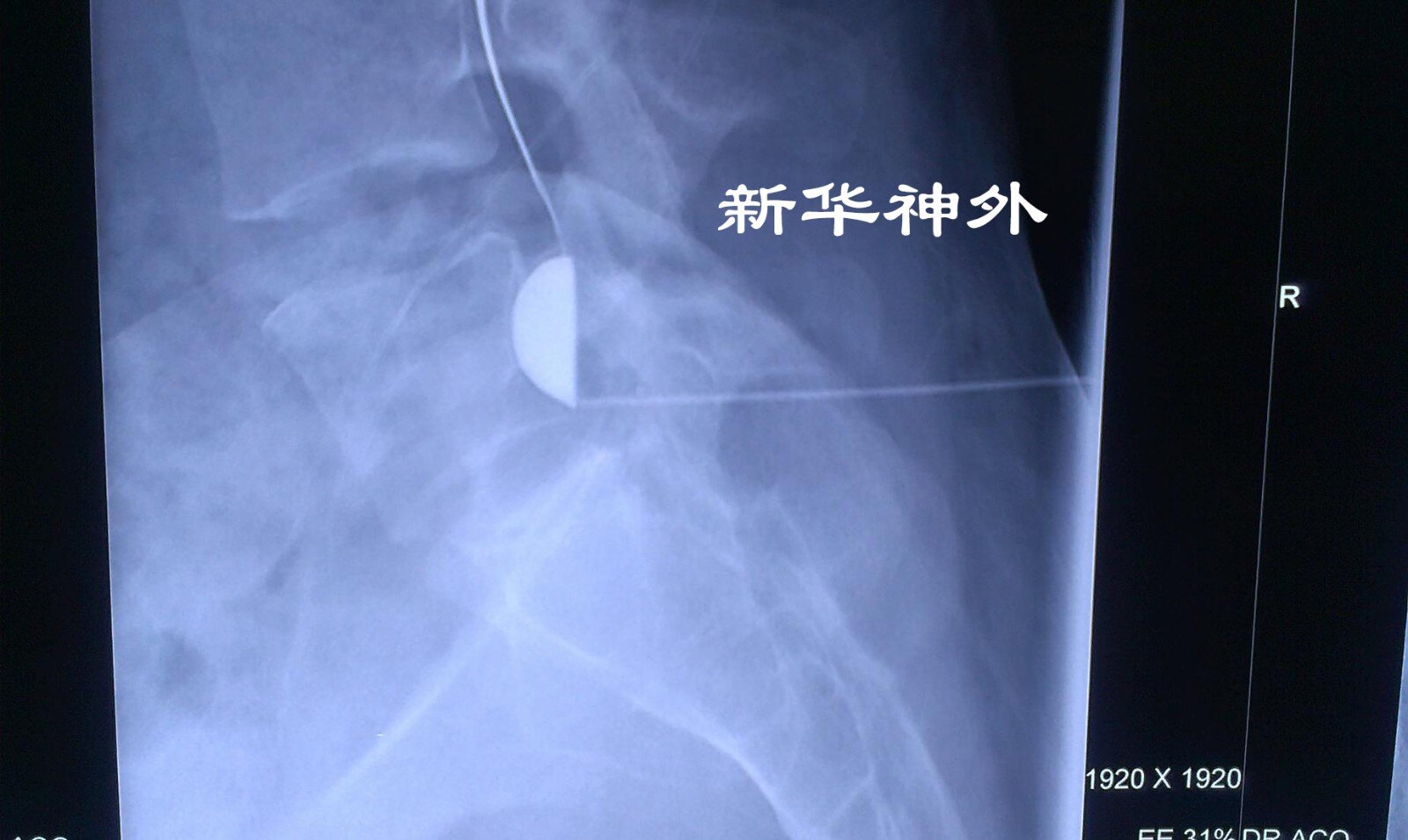
However, the imaging study depicted above illustrates the injection of a contrast agent into a sacral cyst. Upon reaching the level of the leak, the contrast agent promptly escapes and enters the subarachnoid space. Evidently, the aforementioned perspective is incorrect.
Since the leakage in sacral cysts is not a one-way valve but rather a bidirectional flow, allowing for the free movement of fluid in and out, the question arises as to why sacral cysts continue to grow. The answer lies in the high hydrostatic pressure of cerebrospinal fluid in the sacrum when the body is upright, continuously expanding the cyst.
Given that sacral cyst leaks are bidirectional, surgical diversion techniques that open up the sacral cyst and dural sac may exacerbate the condition by increasing the size of the leak and the flow rate.Author Xuesheng Zheng
Posted
A middle-aged female patient has been experiencing sacrococcygeal pain accompanied by numbness in the buttocks for four years. Over the past three months, her symptoms have worsened, particularly when standing or sitting for prolonged periods, but find relief when lying flat. Her urination and defecation remain normal.
Her symptoms are reminiscent of a sacral cyst.
Despite undergoing magnetic resonance imaging (MRI) at multiple hospitals, the diagnosis remained uncertain, with each facility concluding that the imaging findings were similar to a sacral cyst.
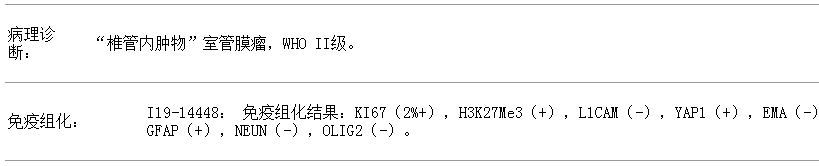
However, Dr. Zheng’s team conducted a thorough review of the images and noticed discrepancies between the MRI signals and those typically associated with a sacral cyst or a sacral cyst with bleeding, which led them to suspect a sacral tumor. They prepared for surgery with two potential diagnoses in mind.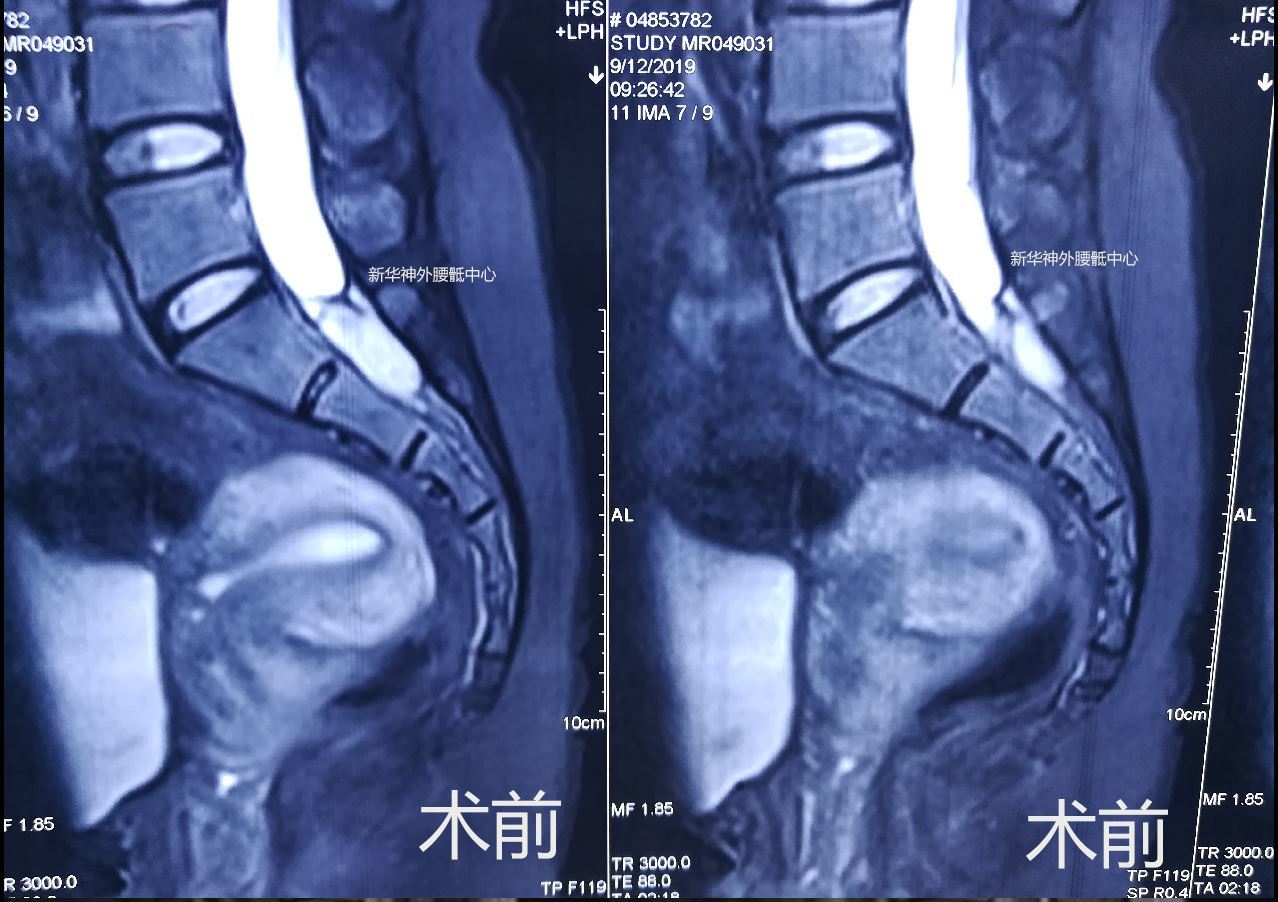
Author Xuesheng Zheng