Health information on Tarlov cyst and relative disorders
Illustration on Minimally invasive surgery for sacral cyst
Posted
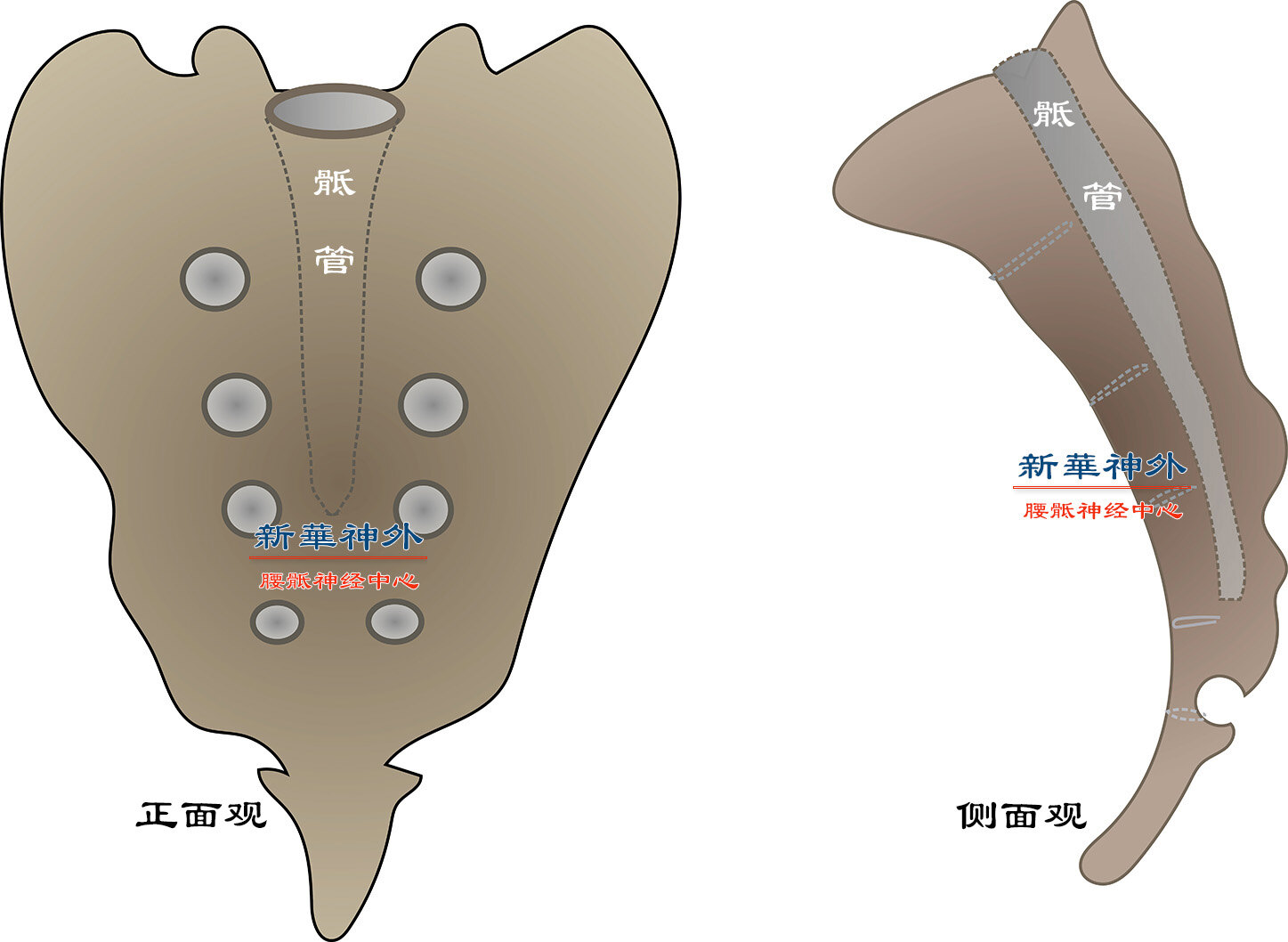
Figure 1: Illustration of the Sacral Canal’s Bony Structure. Positioned posteriorly along the midline of the pelvis, beneath the lumbar spine and above the coccyx, the sacrum comprises five fused segments (S1 to S5). The sacral canal, a bony conduit, resides centrally within the sacrum.
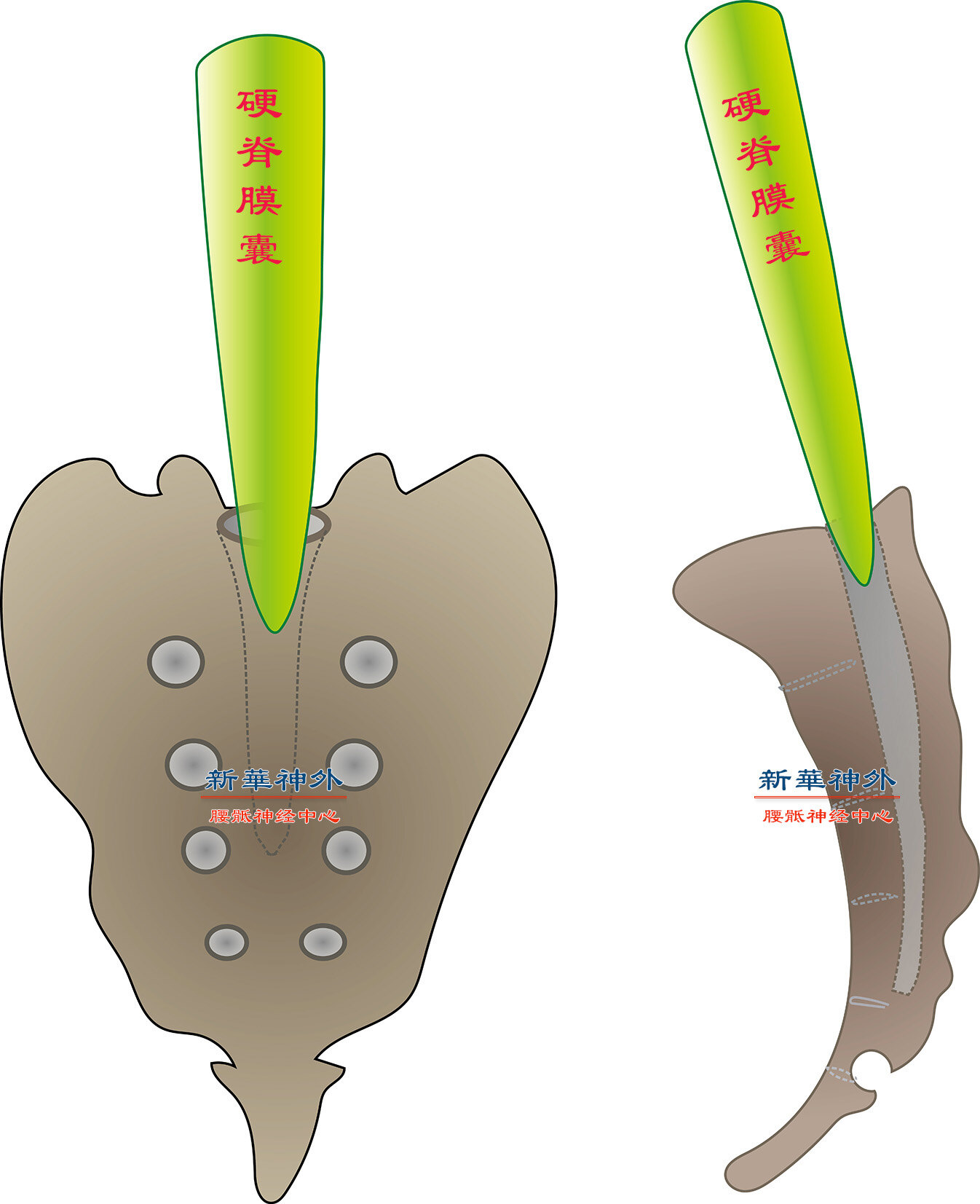
Figure 2: Localization of the Dural Sac’s Bottom. Typically situated at the S1 level, the dural sac connects to the cranial cavity and is filled with cerebrospinal fluid, akin to a tall water bucket. Due to human bipedalism, the static water pressure at the dural sac’s base is quite high, approximately 1/9 of a standard atmospheric pressure.
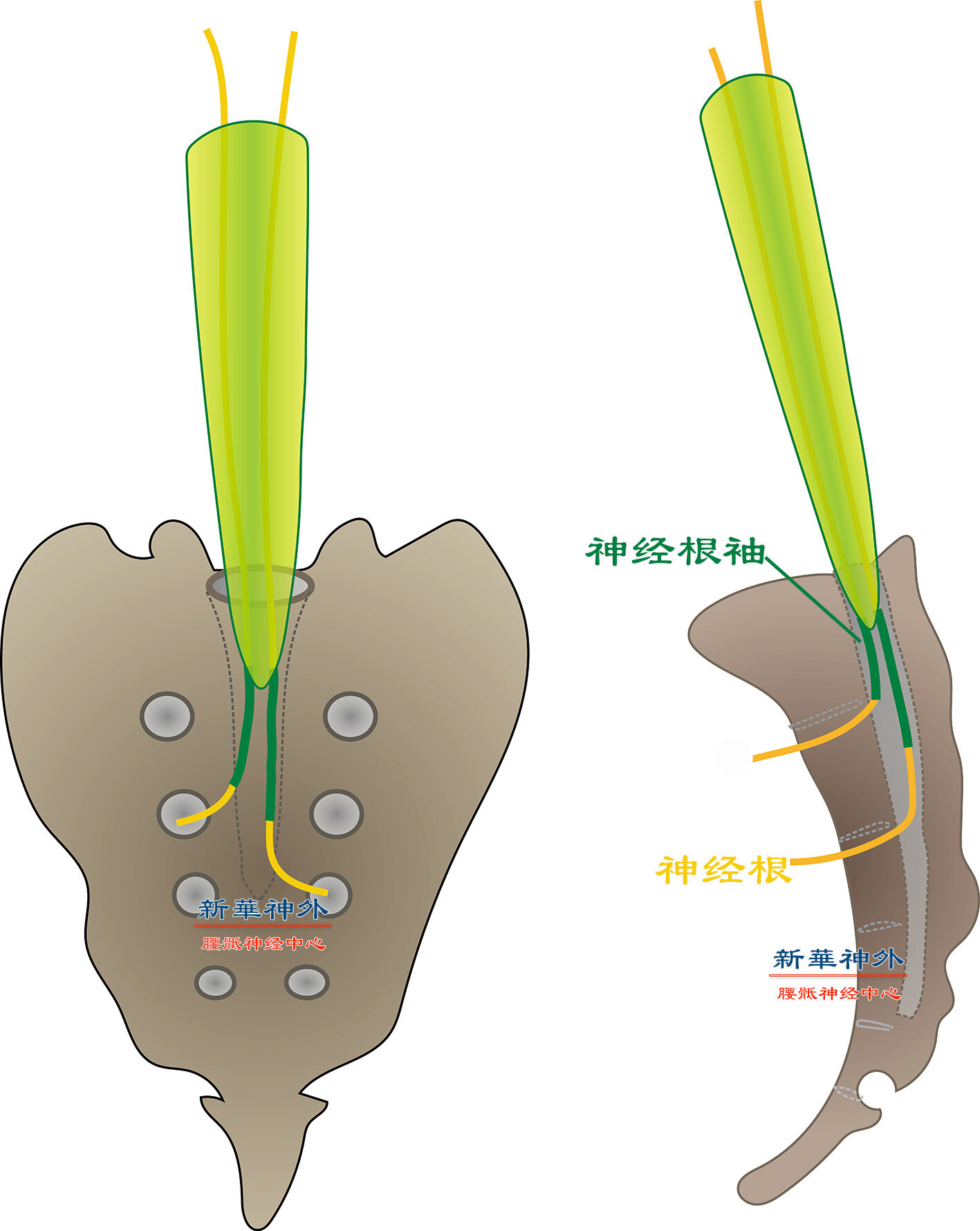
Figure 3: Diagram of Nerve Roots. Inside the dural sac, the nerve root (depicted in yellow) is exposed. Upon emergence, it is enveloped by a layer of dural sac tissue (highlighted in green), which acts as an extension, akin to a sleeve continuing from a garment. Notably, the interior of the nerve root sleeve is devoid of cerebrospinal fluid, resembling a snug-fitting sleeve.
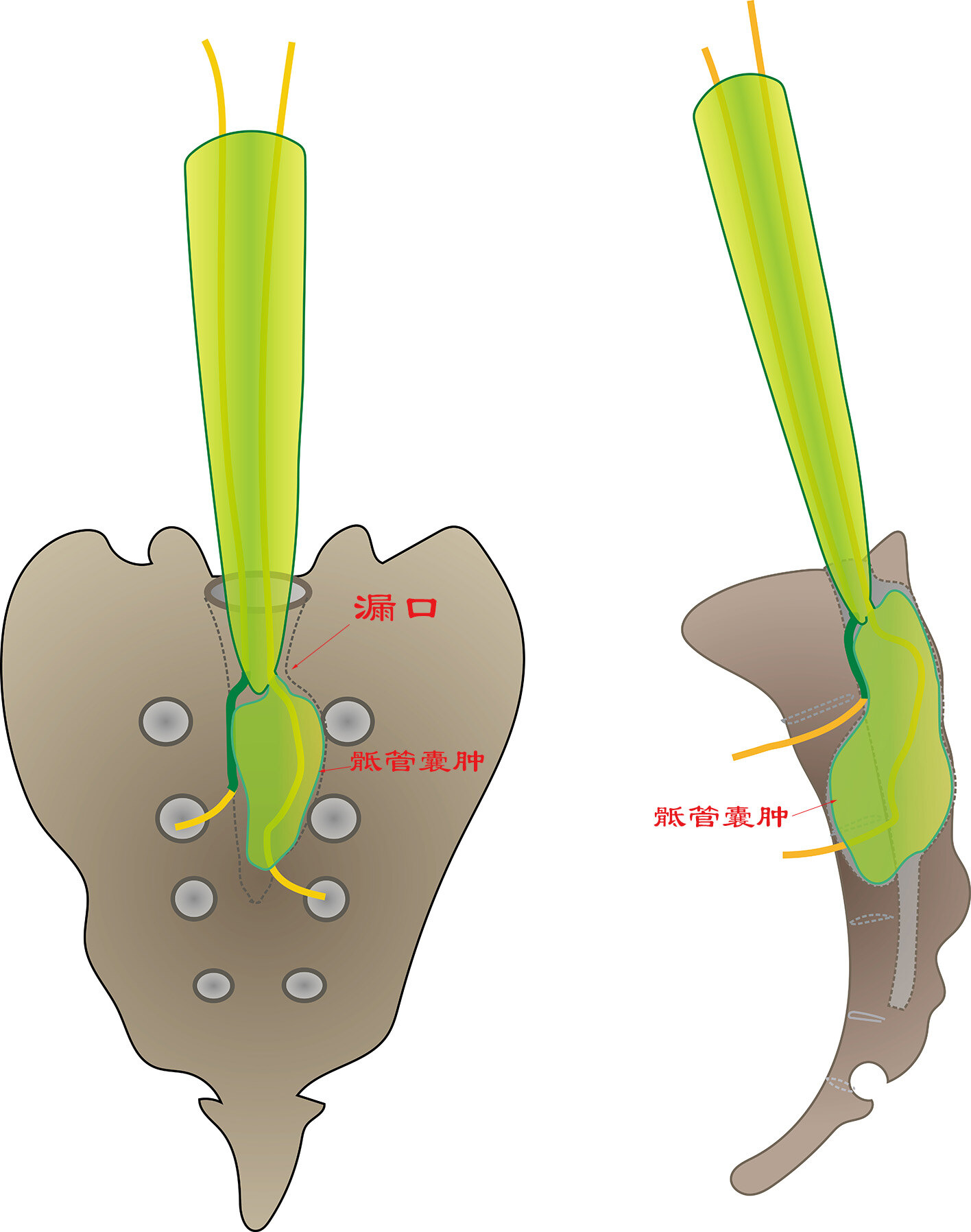
Figure 4: Formation of Sacral Cysts. Congenital weakness at some nerve root’s exit point at the dural sac’s base allows cerebrospinal fluid, under immense pressure, to push into the nerve root sleeve. This expansion leads to the enlargement of the bony sacral canal. Simultaneously, the cyst’s internal nerve roots are stretched, while adjacent external nerve roots are compressed, resulting in pain and urinary and fecal dysfunction. It’s evident that a sacral cyst is not a real cyst or a tumor but rather a cerebrospinal fluid leak. Thus, “resecting” a sacral cyst is impossible; only repairing the leak is feasible.
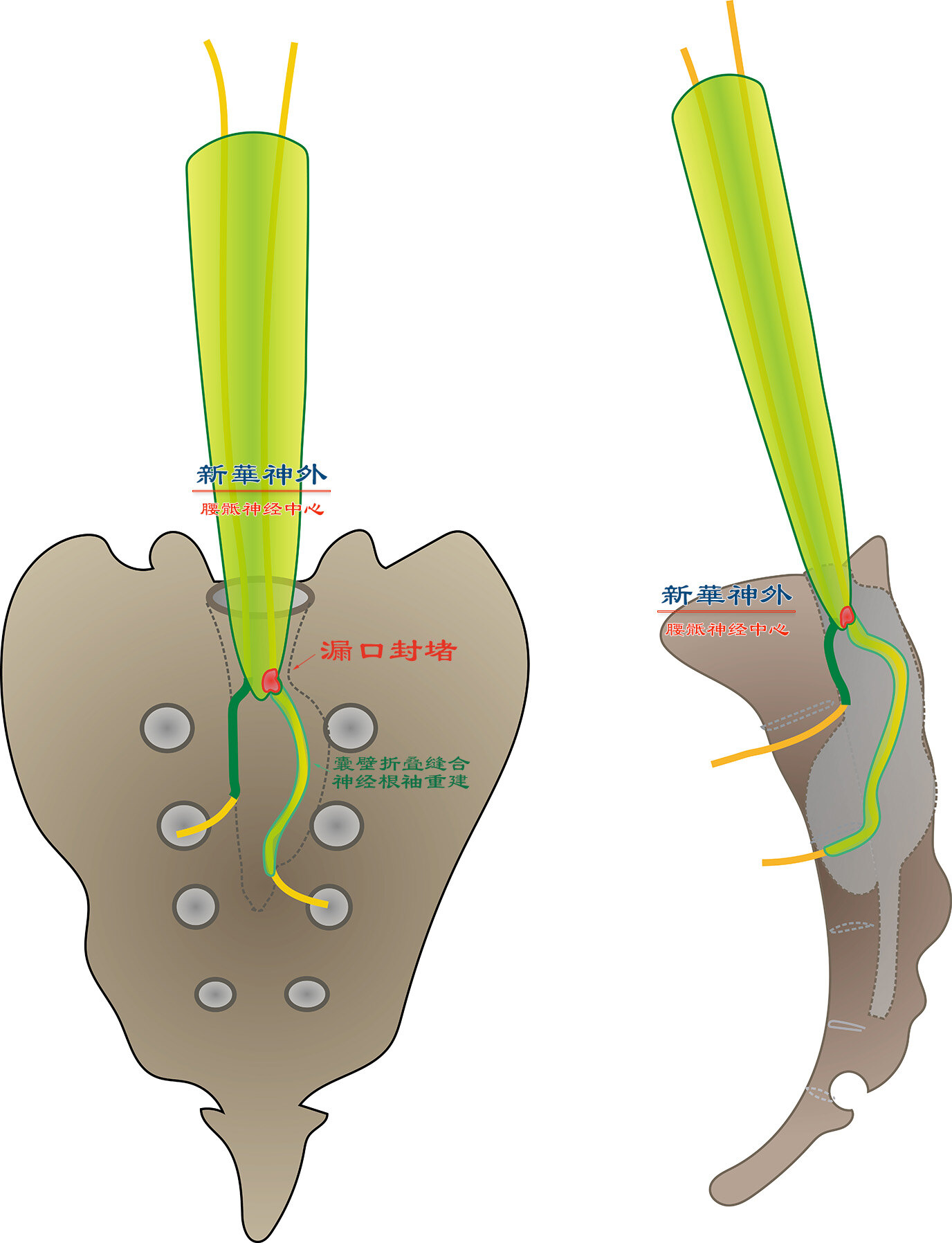
Figure 5: Ideal Surgical Strategy for Sacral Cyst . (1) Given that the disease originates from congenital weakness at the nerve root sleeve’s exit, which cerebrospinal fluid enlarges into a leak, the core surgical technique involves using micro suturing to block the leak with a small muscle fragment without harming the traversing nerve root. (2) Cerebrospinal fluid enlarges the nerve root sleeve (i.e., cyst wall). Post-successful occlusion, cerebrospinal fluid within is aspirated to confirm no further leakage. At this juncture, the cyst wall is folded, wrapped around the nerve root, returning it to a snug-fitting sleeve.
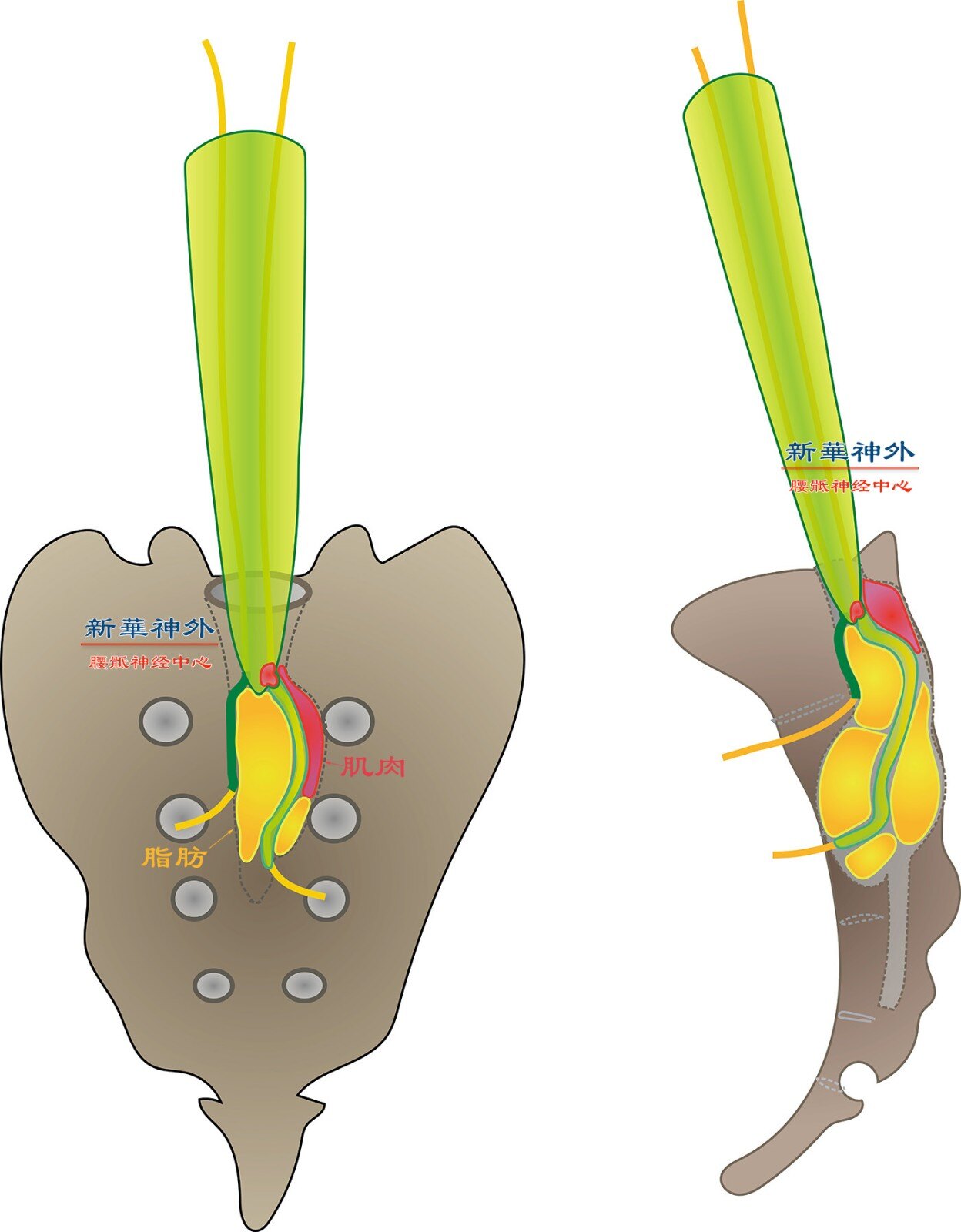
Figure 6: Addressing an Enlarged Bony Sacral Canal. Since bone regeneration is impossible, autologous muscle and fat are utilized to fill the bony sacral canal, as adipose tissue naturally resides there under physiological conditions. Consequently, post-sacral cyst surgery, magnetic resonance imaging reveals fat and muscle. After several months, slight fat liquefaction results in a subtle liquid signal on imaging.
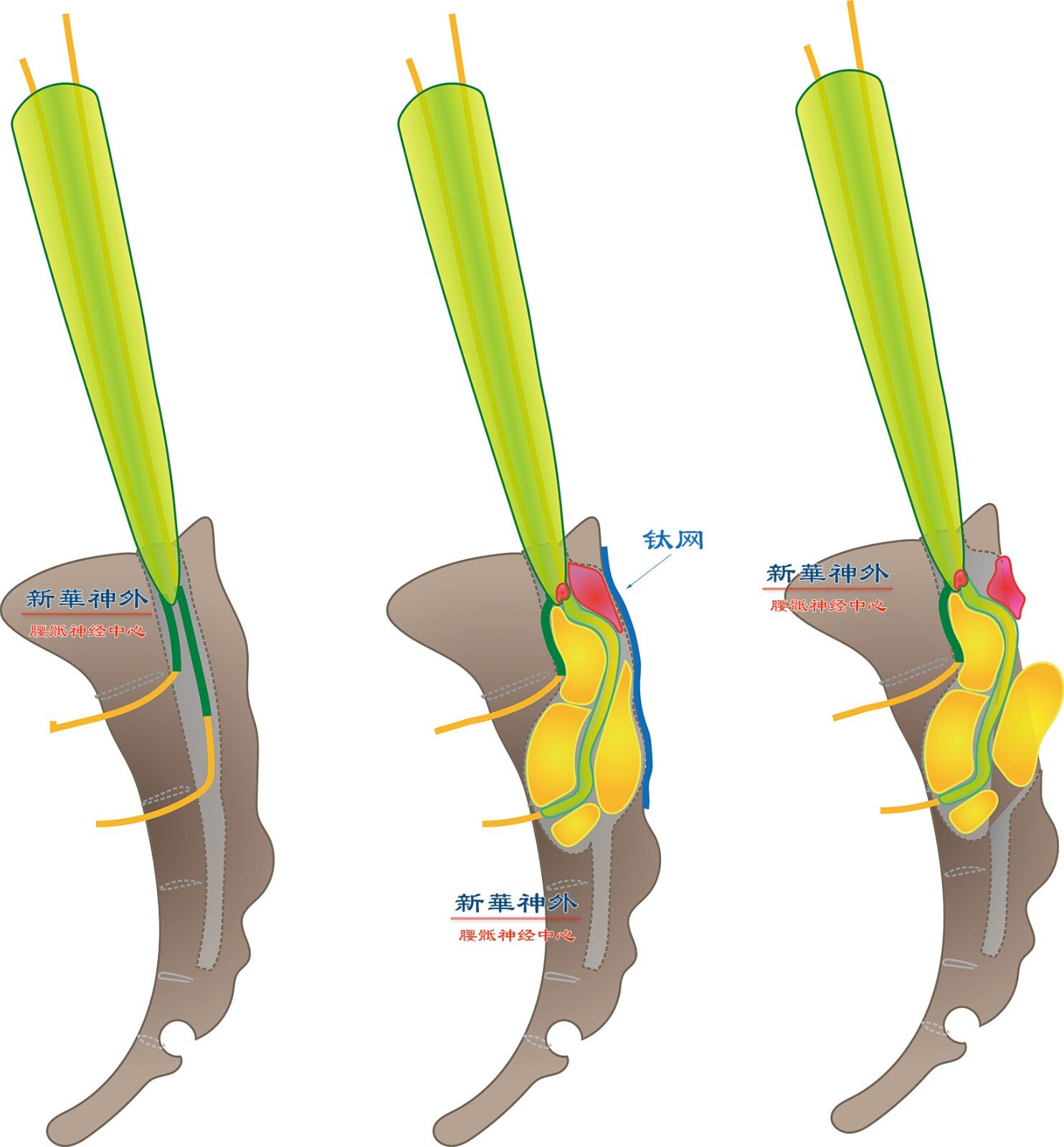
Figure 7: Surgical Conclusion with Titanium Mesh Application. To prevent sacral canal content protrusion, titanium mesh should be employed to repair the sacral canal’s posterior wall.