Clinical manifestations: Anal and perineal pain, weakness in urination and defecation
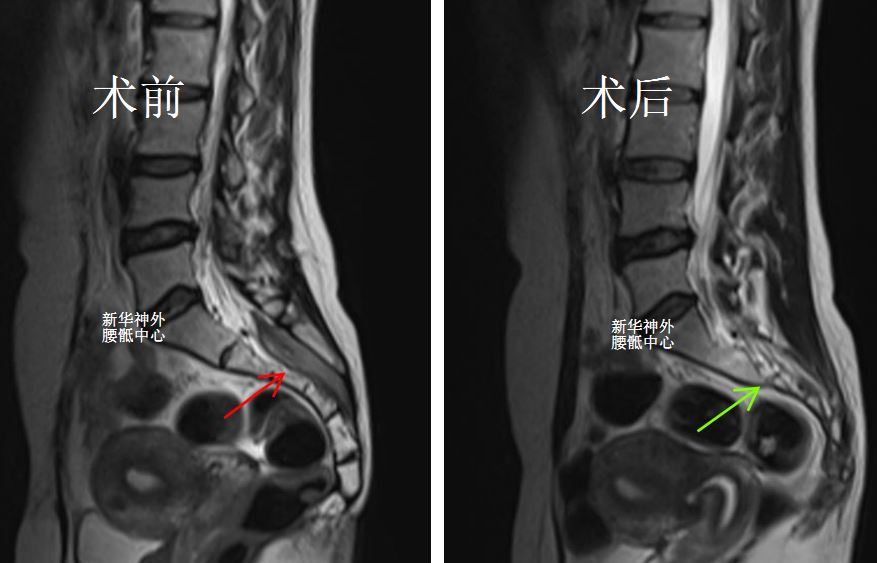
Preoperative magnetic resonance imaging showed a tumor (red arrow) in the sacral canal, ranging from S1-S4, approximately 7cm long, surrounding the cauda equina nerve root.
Dr. Zheng’s team from the Neurosurgery Department of Xinhua Hospital affiliated with Shanghai Jiao Tong University School of Medicine performed surgical resection. During the operation, it was found that the tumor was yellowish, with a tough texture and moderate blood supply. Under intraoperative neurophysiological monitoring, the tumor in the sacral canal was resected through microsurgery, while protecting the cauda equina nerve root.
Postoperative bowel function is normal and symptoms disappear.
Postoperative magnetic resonance imaging showed that the tumor in the sacral canal had been totally resected, and the course of the cauda equina nerve root was good (green arrow).
A 65-year-old female patient presented with sacrococcygeal pain, discomfort in the perineum, and incomplete urinary incontinence. This incontinence was exacerbated by coughing or sneezing, causing urine leakage that significantly impacted her daily life and social activities. Additionally, urinary leakage occurred whenever she experienced perineal pain.
A magnetic resonance imaging (MRI) examination conducted at other hospital revealed the presence of a sacral cyst, prompting the patient to seek surgical intervention at our hospital. During the surgery, it was discovered that the sacral cyst had a high-flow leakage and high internal pressure. The cyst was successfully sealed, and the surgery proceeded smoothly.
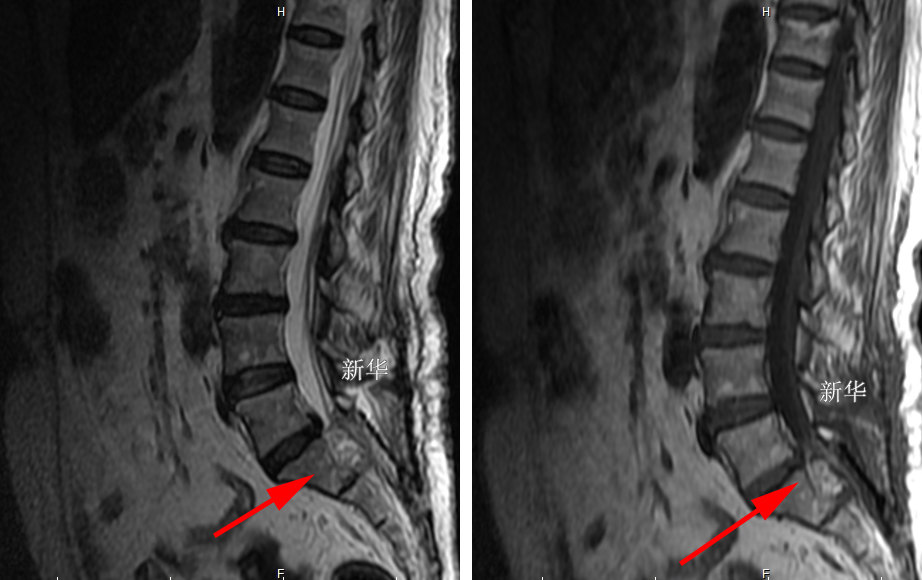
Postoperative MRI confirmed the satisfactory closure of the sacral cyst, as indicated by the red arrow.
Upon discharge, the patient did not experience significant improvement in her urinary incontinence. However, after a period of rest, her urinary incontinence had virtually disappeared two months post-surgery.
Dr. Zheng’s team successfully conducted a surgery to treat a sacral cyst in a middle-aged female patient who initially complained of pain and soreness in the anal region. Subsequently, she developed incomplete anal incontinence, characterized by leakage of fecal fluid but retention of solid stool.
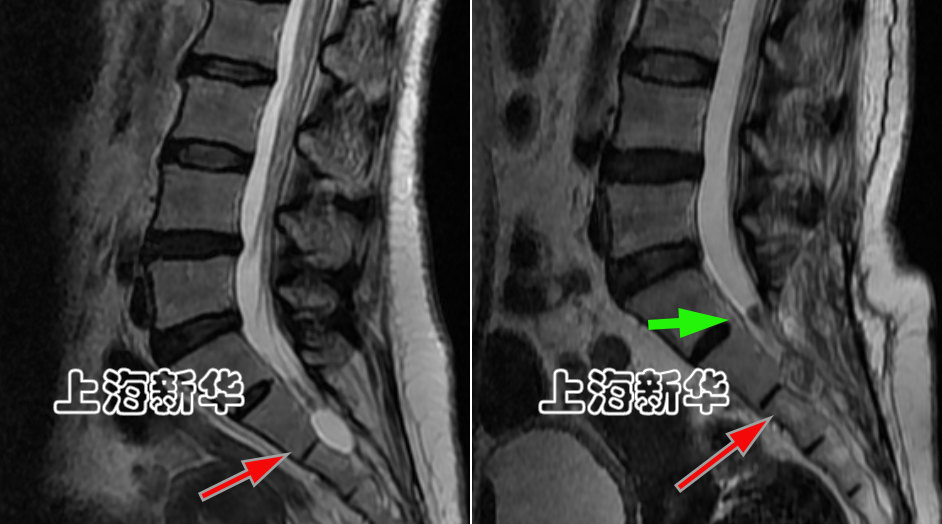
The preoperative magnetic resonance imaging is depicted on the left, while the postoperative imaging is shown on the right. The red arrow highlights the location of the sacral cyst, and the green arrow indicates the sealed leakage.
After a three-month outpatient follow-up, the patient reported complete resolution of her anal incontinence and perianal pain. However, she still experiences mild discomfort in her buttocks and lower limbs.
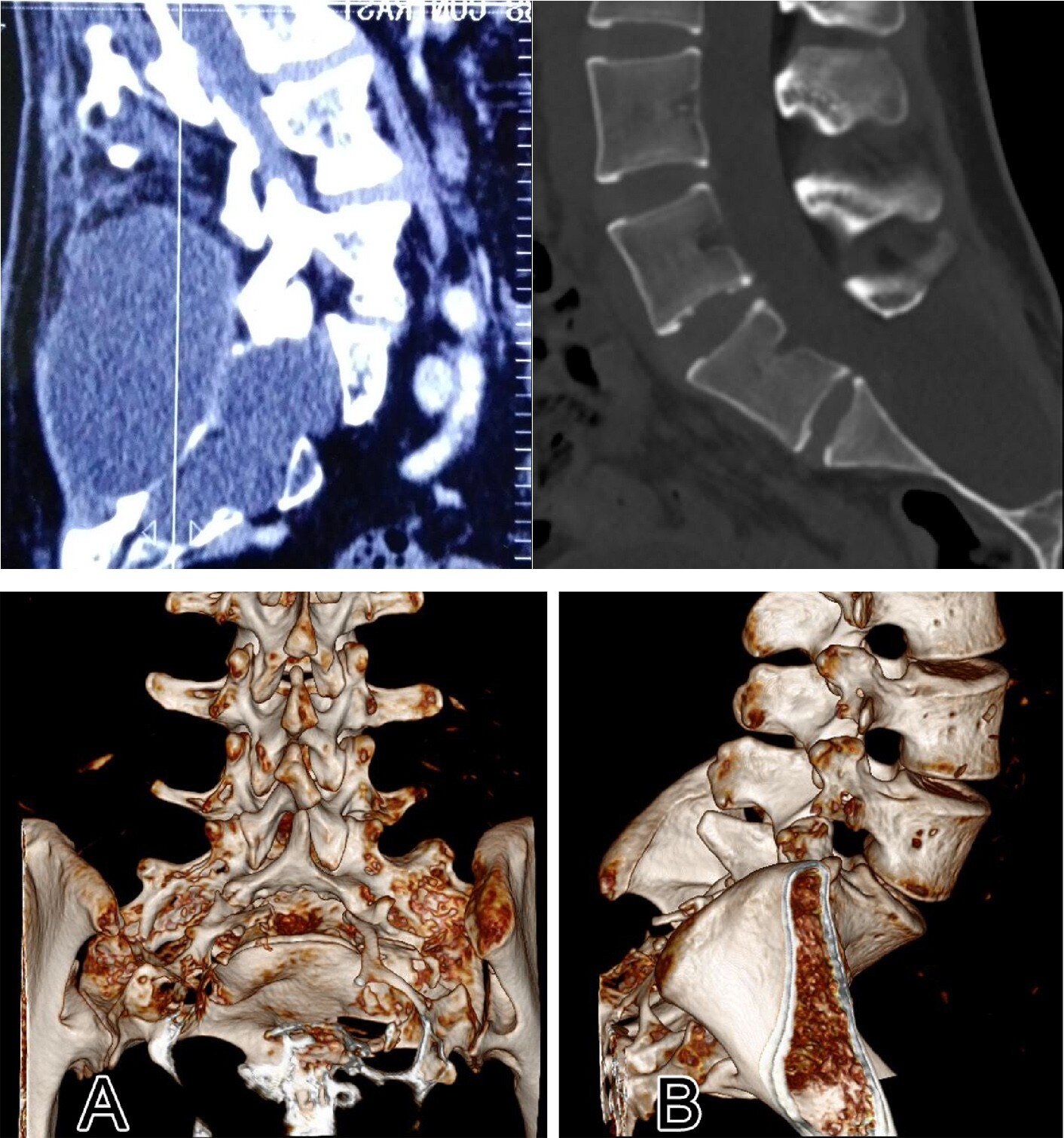
Sacral cysts, due to their expansive growth, have varying degrees of erosion on the sacrum bone. In severe cases, they can penetrate through the sacrum lamina or vertebral body.
Since the disease has damaged the sacrum, during surgery, the remaining sacrum bone should be maximally protected and repaired, which is an important part of the minimally invasive concept of sacral cyst.
As depicted in the figure, the postoperative CT scans of two conventional surgical procedures reveal that the sacral lamina was nearly entirely resected. Consequently, the patient’s inability to maintain an upright posture post-surgery was attributed to the loss of the sacral lamina’s capacity to withstand high hydrostatic pressure. Standing for more than five minutes resulted in severe pain, necessitating immediate recumbency. In extreme instances, protrusion of the spinal membrane could ensue. Consequently, this traditional surgical approach has been discontinued.
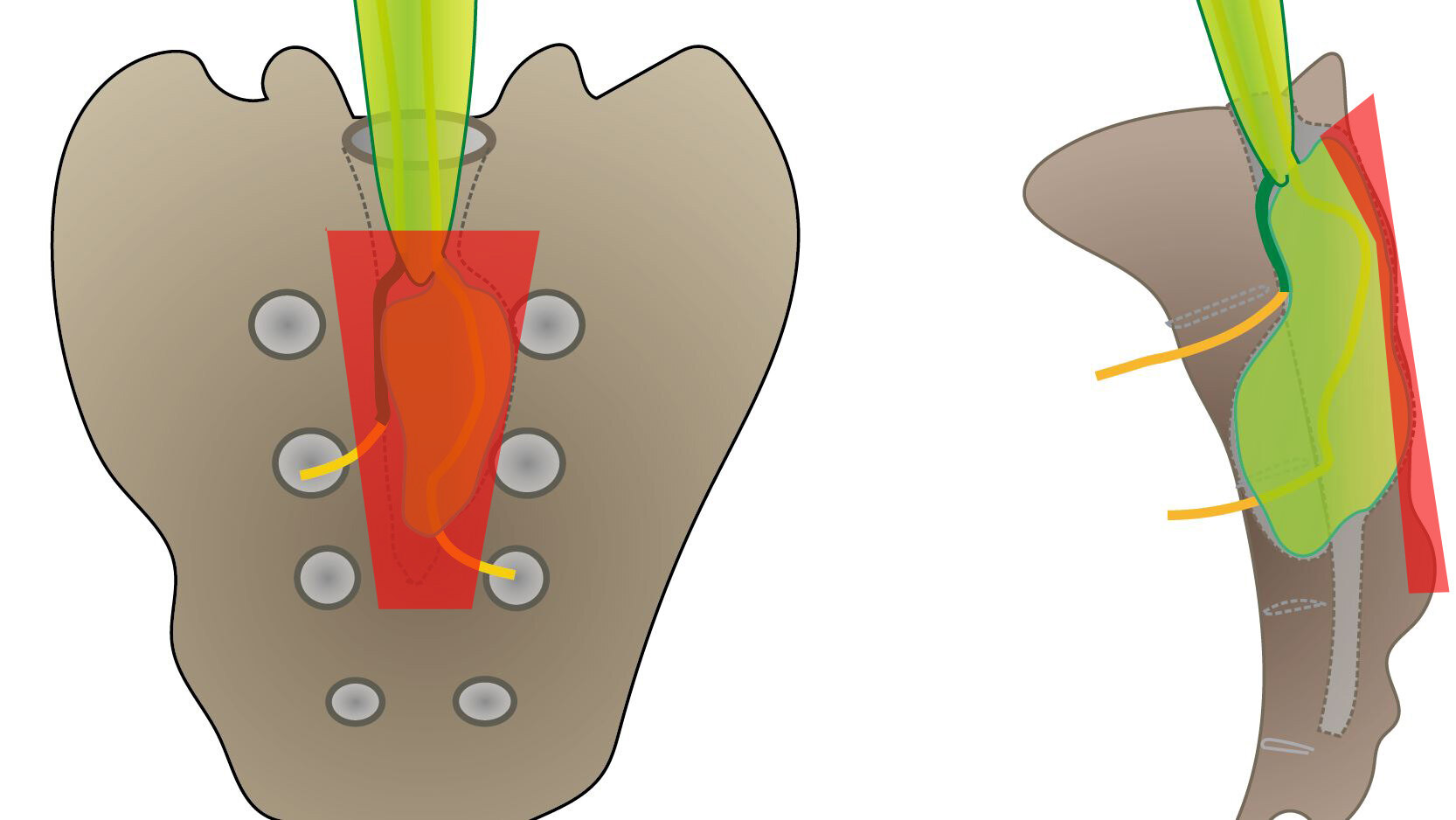
As depicted in the figure below, this represents the surgical method involving gross laminectomy, which was reported in the literature ten years ago. The procedure entails sawing off the lamina surrounding the sacral cyst, followed by utilizing titanium connectors and screws to reposition and stabilize the detached lamina at the conclusion of the surgery. The red area denotes the approximate 3×5cm area of sacral lamina incision. Despite the lamina eventually being repositioned, the bone wound remains substantial, with a noticeable width of the saw groove post-repositioning.
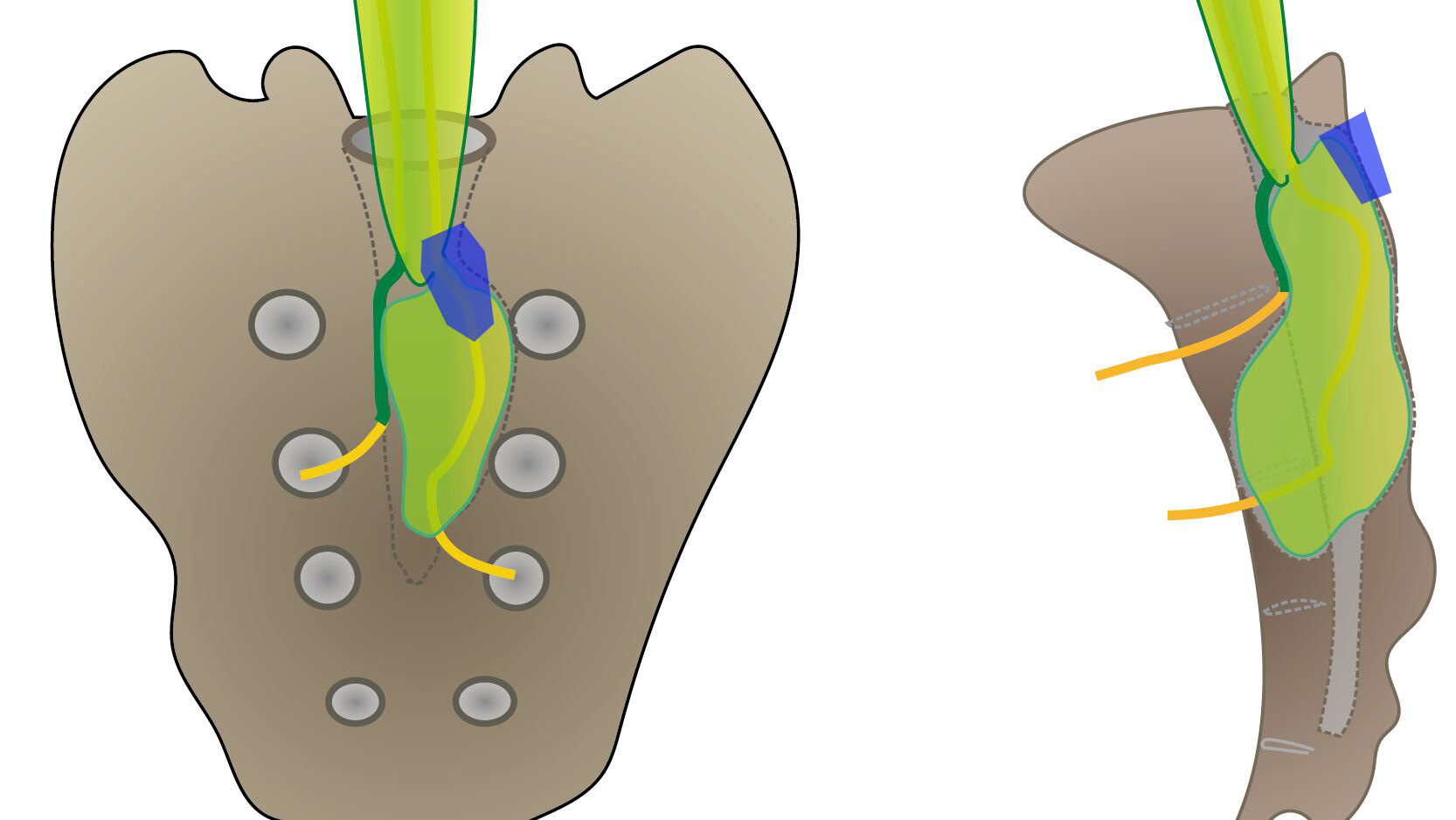
Dr. Zheng’s team has been utilizing a minimally invasive bone window surgery technique, as illustrated in the figure below. The bone incision area measures approximately 1cm, eliminating the need to expose the entire extent of the sacral cyst. By merely exposing the leak at the neck of the cyst, the sacral cyst leak can be effectively sealed. Even in cases where some sacral cysts exceed ten centimeters in length, the surgical bone incision remains minimal, spanning approximately 1.5 centimeters. At the conclusion of the surgery, this small bone window is repaired using a titanium mesh, which measures only about 2cm in diameter. This approach maximizes bone protection, thereby facilitating patients’ timely return to work post-surgery.
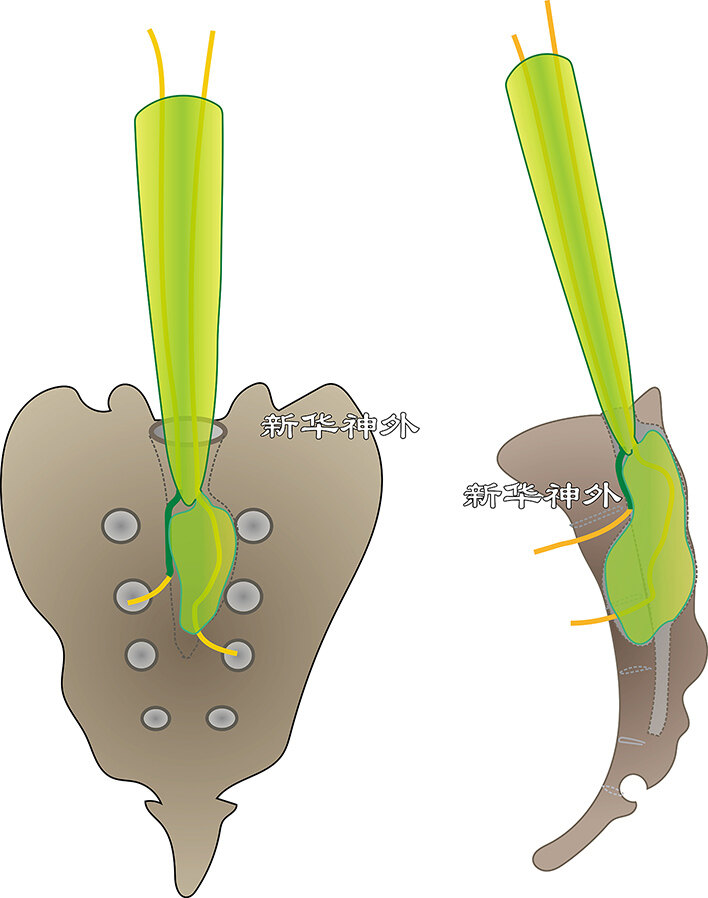
The majority of sacral canal cysts are traversed by a nerve root, with the cervical leak serving as the point of exit for this nerve root from the dural sac. Consequently, the surgery for sacral canal cysts, particularly the crucial step of sealing the leak, must be meticulously conducted in close proximity to the nerve root.
Due to the important functions of the sacral nerve root, including urination and defecation, sexual function, and lower limb motor sensation, the sacral nerve root should not be damaged during surgery. The following is the experience of Dr.Zheng’s team.
1. The surgery must be performed under a clear microscopic field of view. If the blood and flesh are blurry, it may be difficult to see the nerves clearly and accidentally injure them.
2. Performing a total laminectomy of the sacral canal is not advisable due to its irregular shape. Such procedures may result in more bone wound and inadvertently harm nerves. Furthermore, the bone wound created during a total laminectomy increases the likelihood of bleeding, which can obscure the surgical field and compromise visibility.
3. Try to control the amount of bleeding inside the sacral canal as much as possible. If there is a large amount of bleeding, the process of stopping bleeding can also easily damage nerves.
4. For cyst leaks with nerve roots passing through, the cyst neck cannot be ligated, and the leak can be sealed by microsurgical suturing. It is necessary to tightly seal the leak, prevent dripping, and ensure that the nerve roots are not damaged.
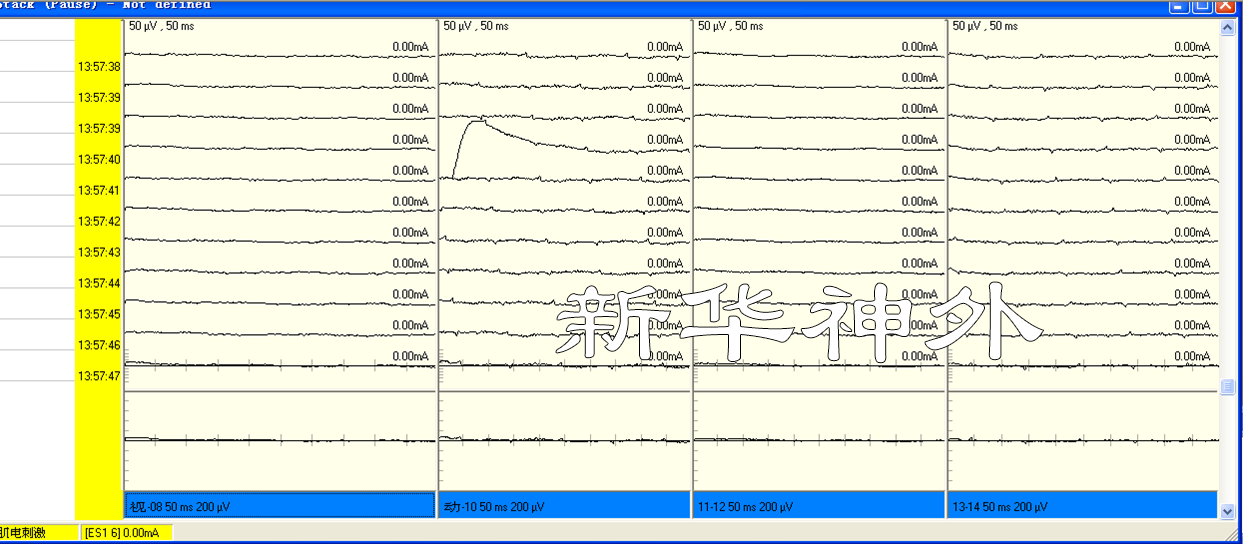
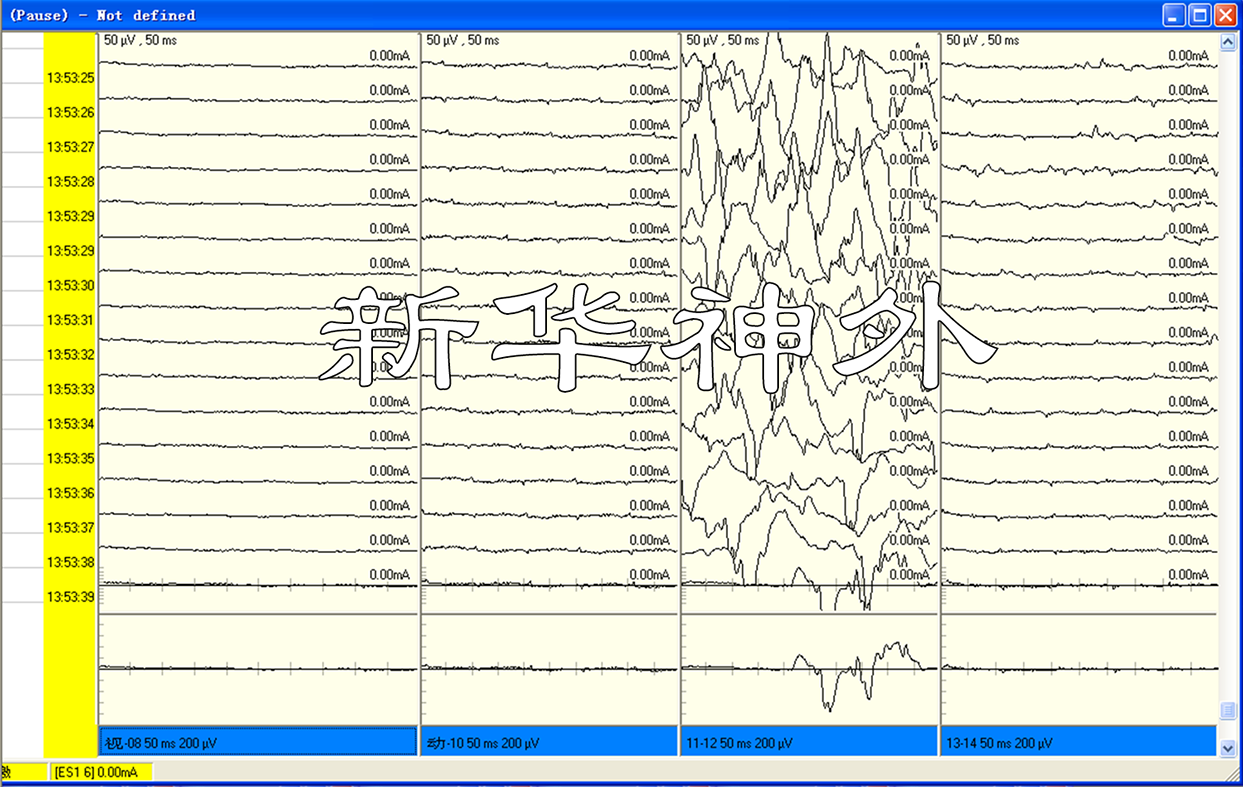
5. Intraoperative neurophysiological monitoring: Needle electrodes are placed around the anus, genitals, thighs, and calves before surgery, and concentric circular electrodes are connected during surgery. Electroencephalography, EMG, SEP, BCR, and other parameters are recorded throughout the surgery to ensure that the nerves are not damaged.
EMG: Resting state
EMG: nerve contact status
Only by strictly following the above principles can the safety of the sacral nerve roots be protected.