Health information on Tarlov cyst and relative disorders
Minimally invasive concept for sacral cyst (1) protecting bone
Posted
Sacral cysts, due to their expansive growth, have varying degrees of erosion on the sacrum bone. In severe cases, they can penetrate through the sacrum lamina or vertebral body.
Since the disease has damaged the sacrum, during surgery, the remaining sacrum bone should be maximally protected and repaired, which is an important part of the minimally invasive concept of sacral cyst.
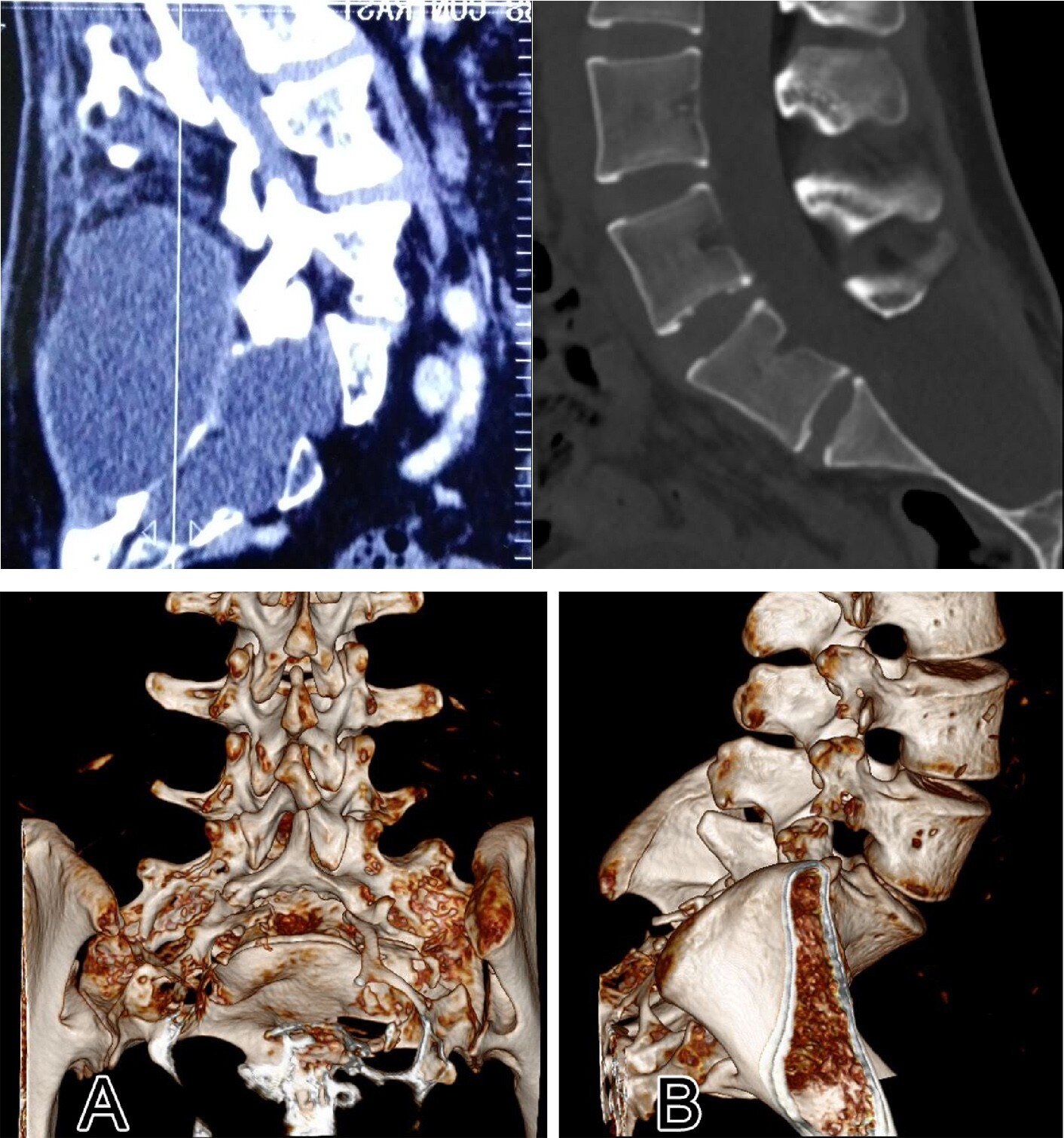
As depicted in the figure, the postoperative CT scans of two conventional surgical procedures reveal that the sacral lamina was nearly entirely resected. Consequently, the patient’s inability to maintain an upright posture post-surgery was attributed to the loss of the sacral lamina’s capacity to withstand high hydrostatic pressure. Standing for more than five minutes resulted in severe pain, necessitating immediate recumbency. In extreme instances, protrusion of the spinal membrane could ensue. Consequently, this traditional surgical approach has been discontinued.
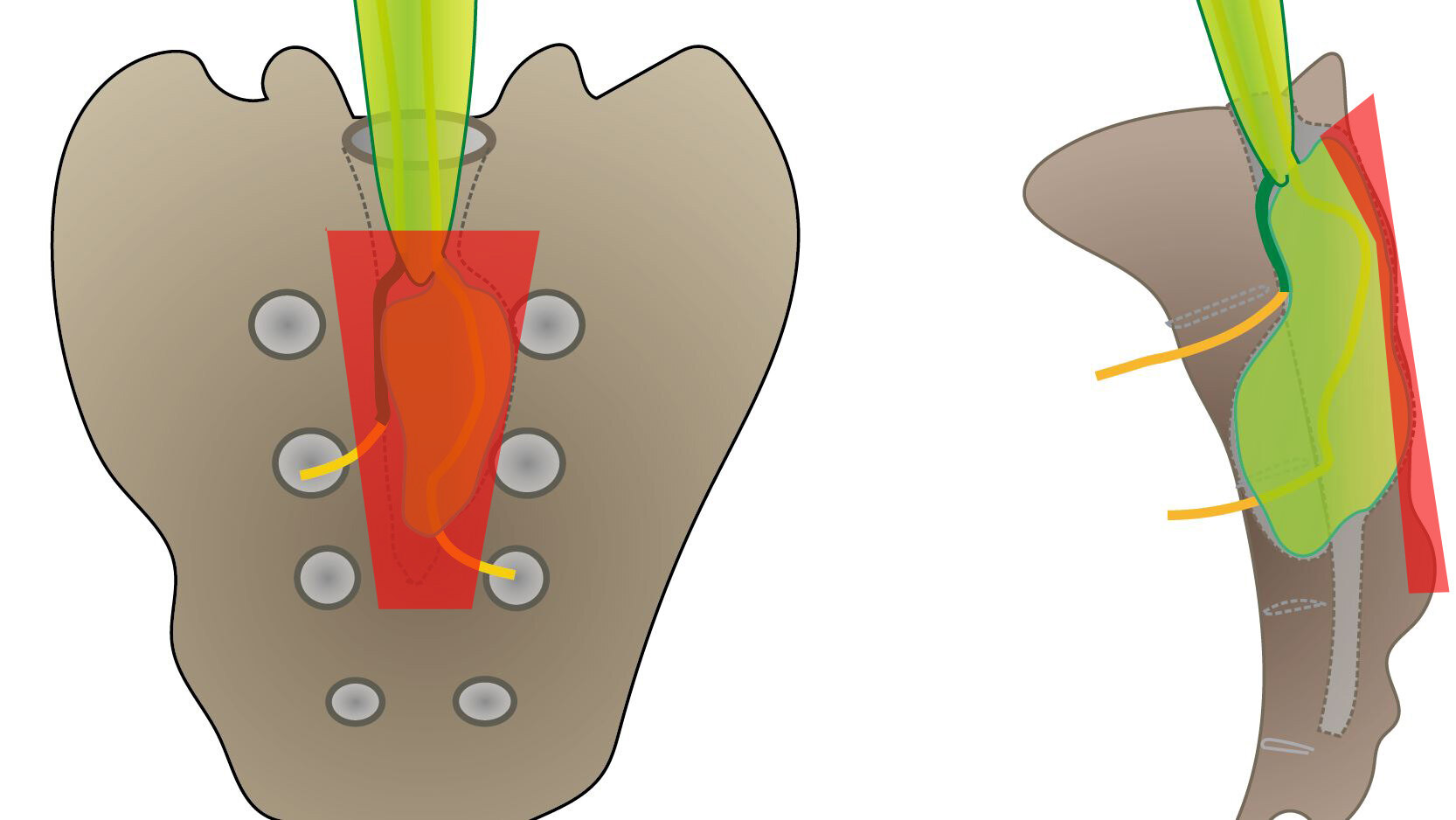
As depicted in the figure below, this represents the surgical method involving gross laminectomy, which was reported in the literature ten years ago. The procedure entails sawing off the lamina surrounding the sacral cyst, followed by utilizing titanium connectors and screws to reposition and stabilize the detached lamina at the conclusion of the surgery. The red area denotes the approximate 3×5cm area of sacral lamina incision. Despite the lamina eventually being repositioned, the bone wound remains substantial, with a noticeable width of the saw groove post-repositioning.
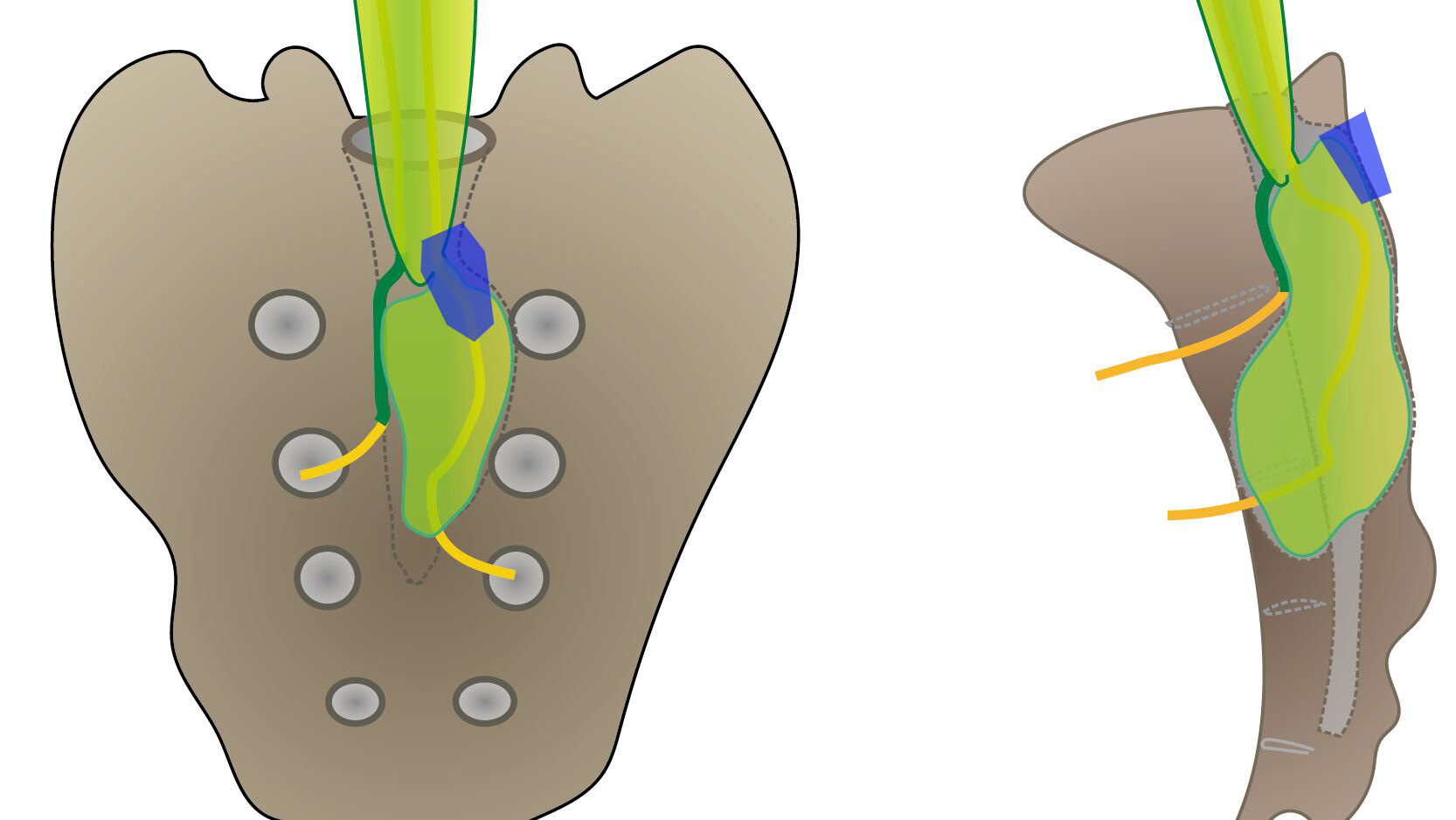
Dr. Zheng’s team has been utilizing a minimally invasive bone window surgery technique, as illustrated in the figure below. The bone incision area measures approximately 1cm, eliminating the need to expose the entire extent of the sacral cyst. By merely exposing the leak at the neck of the cyst, the sacral cyst leak can be effectively sealed. Even in cases where some sacral cysts exceed ten centimeters in length, the surgical bone incision remains minimal, spanning approximately 1.5 centimeters. At the conclusion of the surgery, this small bone window is repaired using a titanium mesh, which measures only about 2cm in diameter. This approach maximizes bone protection, thereby facilitating patients’ timely return to work post-surgery.