The key principles in minimally invasive surgery for sacral canal cysts revolve around nerve root protection and bone preservation, which have been extensively discussed in two prior articles. While the size of the skin incision and the extent of paraspinal muscle dissection are not the paramount factors influencing prognosis, it is nonetheless imperative to optimize these aspects to the fullest extent possible. This ensures minimal postoperative scarring, enhances aesthetic appeal, and mitigates potential long-term impacts.
Here are some experiences of Dr. Zheng’s team:
(1) For sacral cysts less than 5 centimeters, surgery can generally be performed with an incision of about 4 centimeters. Due to the need for microsurgical closure of the leakage during sacral cyst surgery, the 4cm incision cannot be made any smaller, as it cannot allowed suturing.
(2) For huge sacral cysts bigger than 5 centimeters, the incision may need to be larger. If the incision is larger than 6 centimeters, it is generally not recommended to perform intradermal suturing to avoid poor wound healing.
(3) When designing a skin incision, the neck of the sacral cyst should be the center, and the range of paraspinal muscle dissection should also be centered around the neck of the cyst; If the sacral cyst is limited to one side, generally only the paraspinal muscle on the affected side needs to be peeled off, and there is basically no need to peel off the contralateral side.
(4) The outer boundary of paraspinal muscle dissection is the inner edge of the sacral foramen to avoid damaging the sacral posterior branch;
(5) The paraspinal muscle dissection should generally not extend beyond the lower border of L5. This approach offers the advantage of preserving the possibility of future lumbar anesthesia, such as for painless childbirth or cesarean section, through the L3-4 or L2-3 intervertebral spaces. Furthermore, in the event that the patient experiences lumbar disc herniation later in life and requires lumbar surgery, the impact of scar adhesion will be minimal.
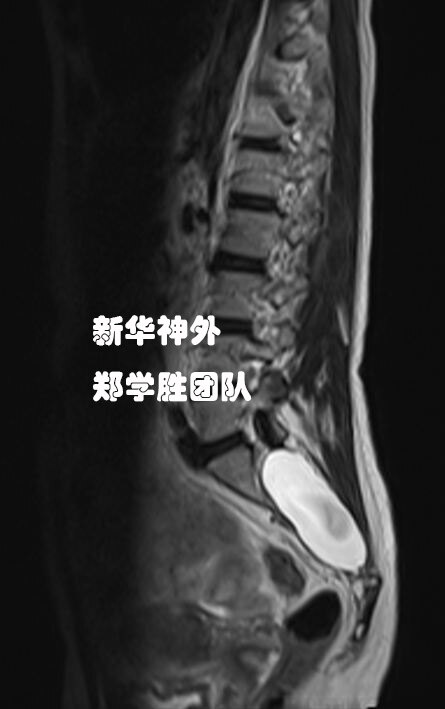
A ten year old child, due to frequent back pain and sometimes difficulty defecating, was found to have a huge sacral cyst on magnetic resonance imaging, extending from the lower edge of L5 to the upper edge of S4.
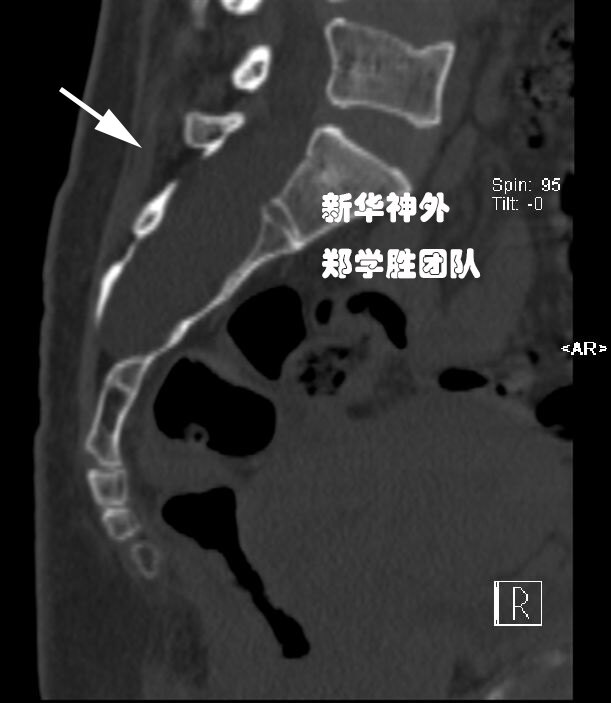
CT scan also revealed spina bifida, with the entire sacral canal cracked open.
Generally, operating on such a large sacral cyst in pediatric patients is challenging due to their typically slender build and lack of fatty and muscular tissue. When surgery is deemed necessary, it is often conducted in two phases: the first involves sealing the leakage to halt the cyst’s growth, followed by a second surgery after the patient has gained weight during adolescence. However, in this particular case, the child is robust and well-nourished, possessing adequate fat and muscle. Therefore, we opted to aim for a successful single-stage surgery.
The surgery progressed exceptionally smoothly, successfully sealing the sacral cyst and repairing the spina bifida. The child’s own spina bifida and sacral cyst had caused significant erosion to the sacral bone, resulting in a severe bone defect. Consequently, we refrained from resecting any additional bone during the surgery and instead fully utilized the bone defect area to complete the procedure. Following titanium plate repair, the postoperative bone structure is now more intact than it was prior to the surgery.
Postoperative magnetic resonance imaging showed complete closure of the sacral cyst. The surgical incision is only 4 centimeters, and the child has almost no pain after surgery. There is no neurological dysfunction.
Dr. Zheng’s observation: The complexity of surgery for large sacral cysts in children is comparable to that in adults. The primary distinction lies in the adequacy of subcutaneous fat and muscle. In thin patients, the surgery often necessitates a two-stage approach. Conversely, in robust patients, a successful single-stage surgery is feasible. Therefore, it is advisable for such children to enhance their nutrition to increase the likelihood of undergoing a successful surgical intervention.
During the surgery, a huge terminal filament sacral cyst was observed with a large leakage flow. After cutting off the terminal filament, the leakage was tightly sealed to ensure no cerebrospinal fluid leakage.
Given the extensive size and significant bone erosion of sacral cysts, there is a bone defect (arrow) approximately 1.5 centimeters in size, allowed for us to perform the micro suturing without the necessity of resecting more bone, thereby maximizing the preservation of the residual sacrum. Postoperatively, reinforcing the bony barrier with titanium plates is essential for achieving long-term therapeutic success.
Postoperative follow-up MRI: The sacral cyst is well sealed. Arrow: The leak has been tightly sealed.
The surgical incision was only 4.5cm, and the patient was discharged two weeks after surgery with symptoms relieved soon.
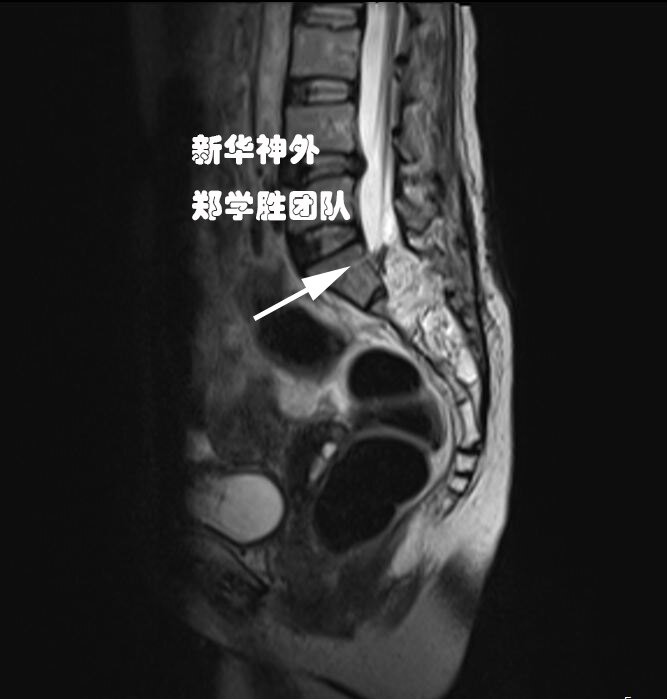
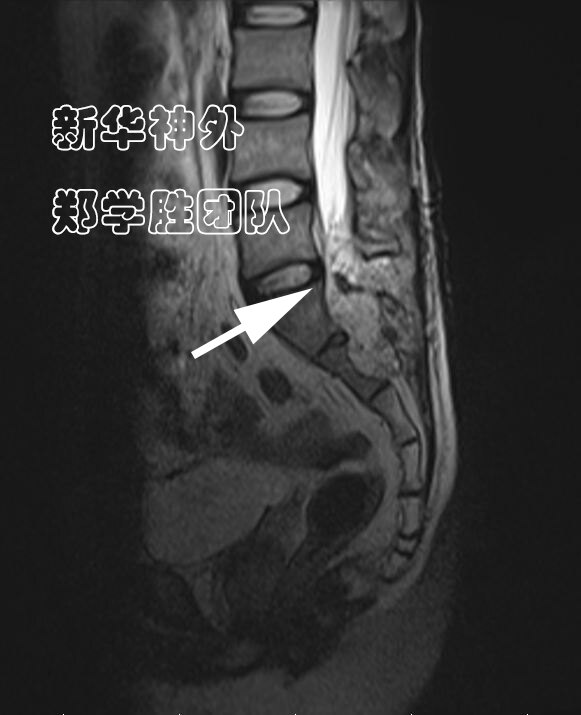
Middle aged male, with pain in the lumbar, sacral, and caudal regions for 1 year, accompanied by soreness of the anus and perineum.
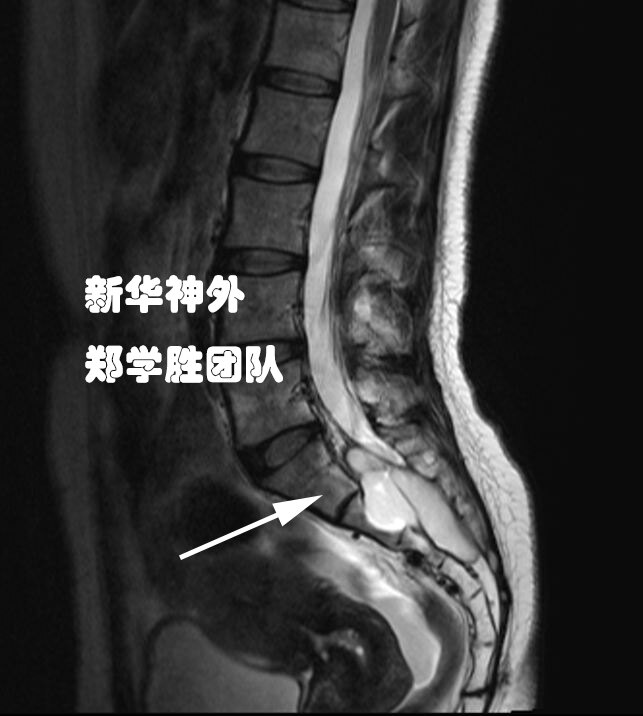
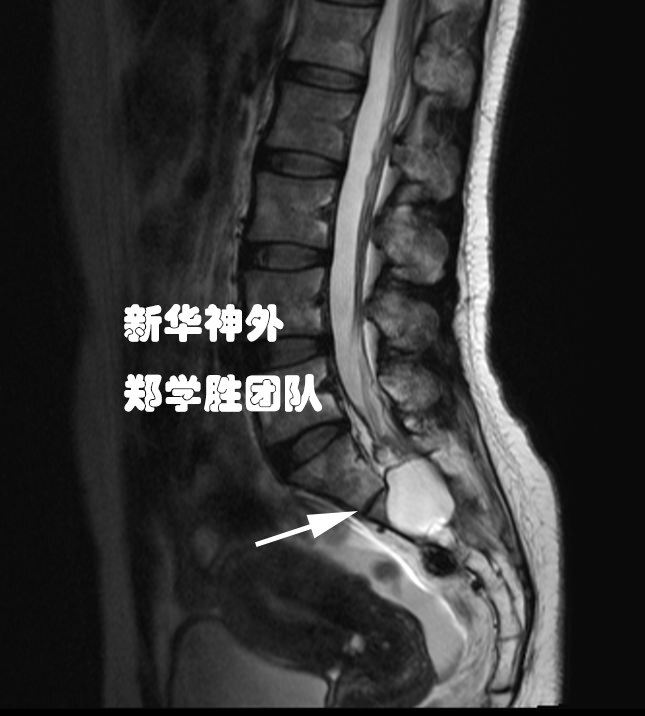
Preoperative MRI showed a 8cm lumbar-sacral cyst.
Since water flows downwards, is the leak located in the upper part of the L5?
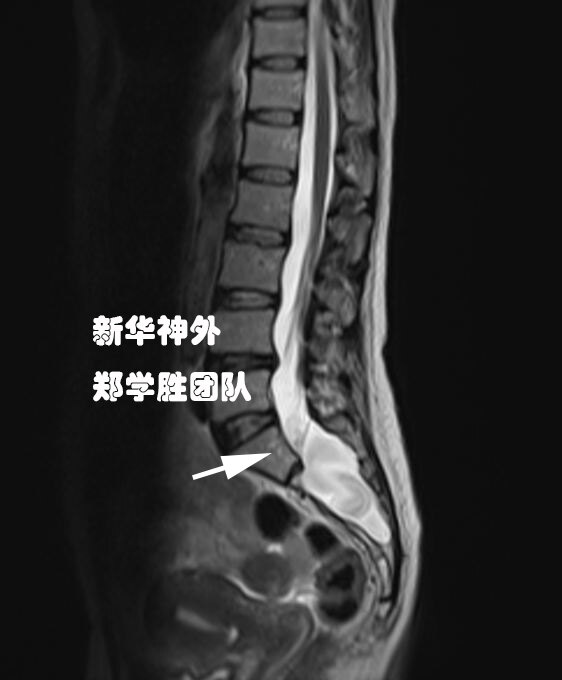
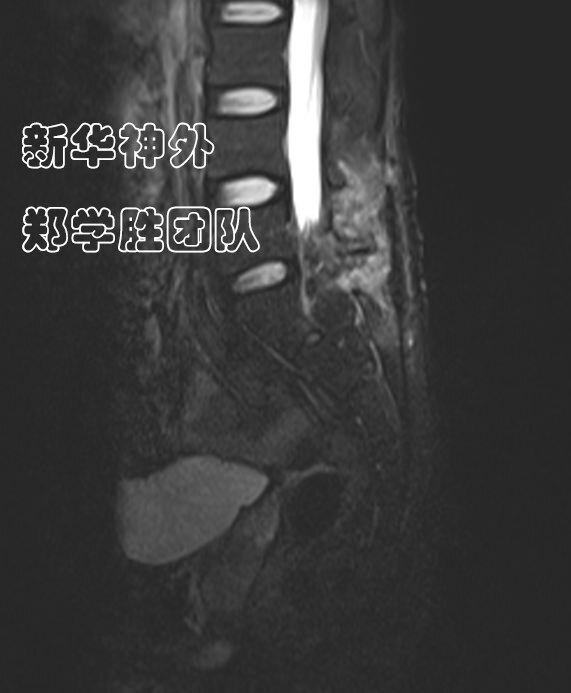
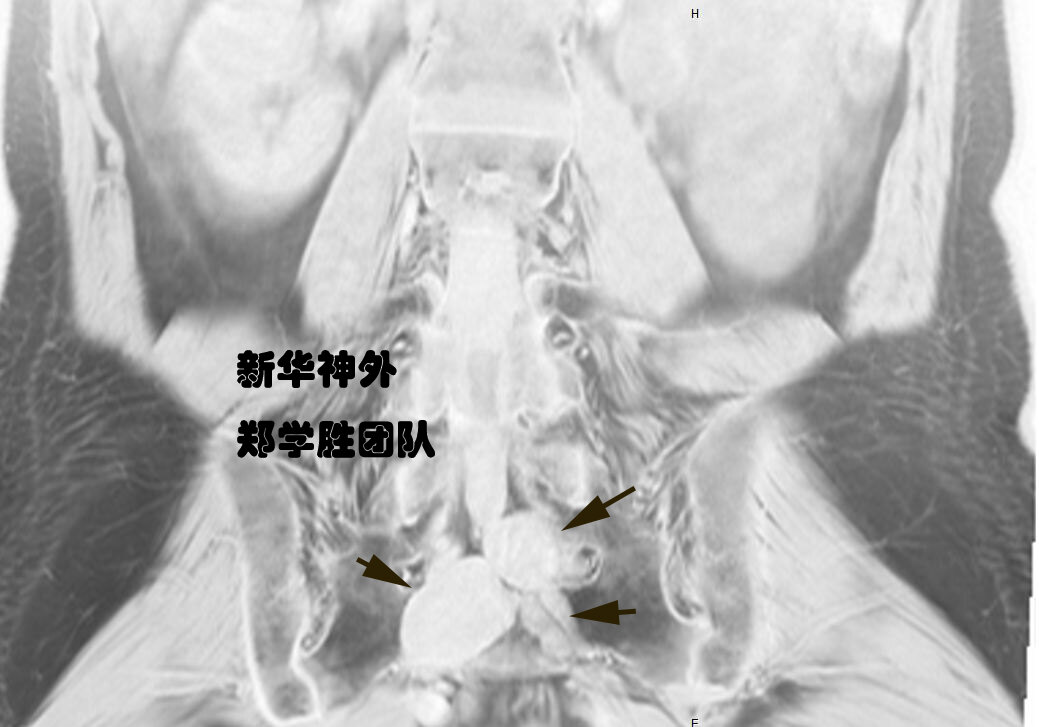
After careful reading of the images, Dr. Zheng determined that the leakage of the lumbar-sacral cyst is located in the gap between L5 and S1 (indicated by the arrow), rather than in the mid L5 region.
Based on this judgment, a 5cm small incision was made, and during the operation, a cerebrospinal fluid leak was indeed found in the L5-S1 space, which was a nerve root cyst. It was sealed without any leakage. Due to the surgery being performed entirely in the L5-S1 space, the bone mass of the lumbar and sacral vertebrae was not resected, making it very minimally invasive.
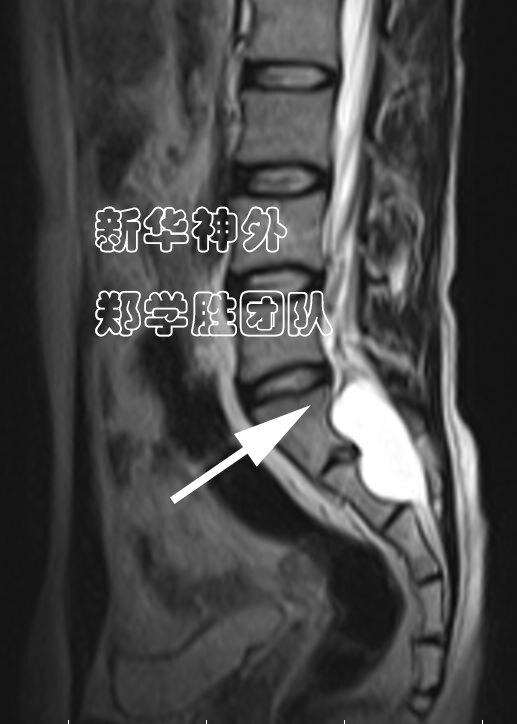
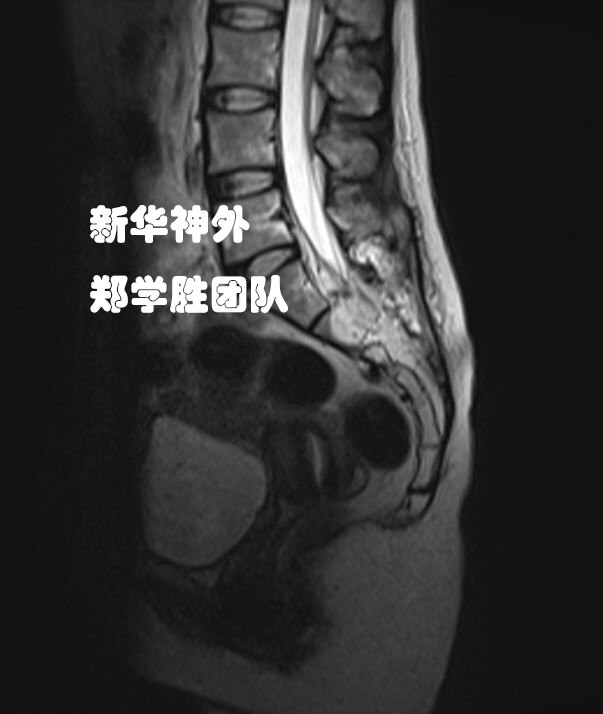
Postoperative follow-up MRI: The leak (indicated by the arrow) is completely sealed.
A young female has been experiencing pain in her lumbar and sacral regions for over a year, with her symptoms progressively worsening. Prolonged sitting and fatigue exacerbate her condition, whereas rest brings some relief. Her urination and defecation functions remain normal.
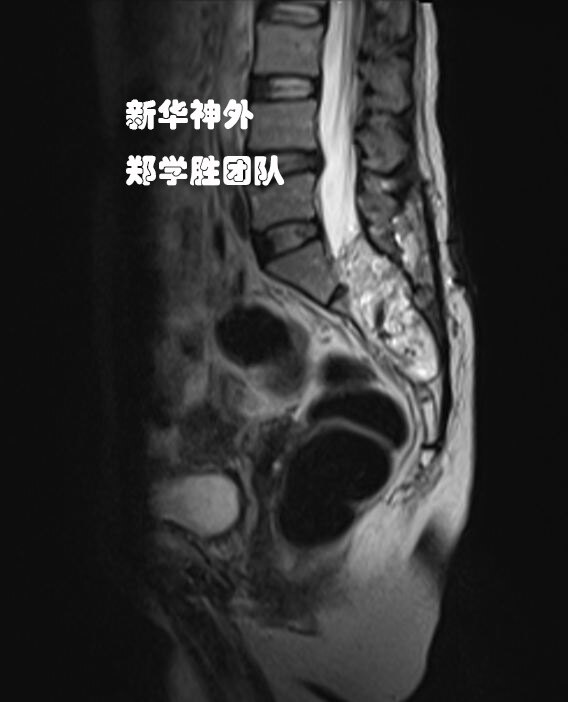
MRI: Multiple sacral cysts.
CT scan shows severe bone erosion.
Three large sacral cysts were identified and securely sealed. Following the surgery, the patient’s symptoms are gradually improving and she is in the process of recovery.