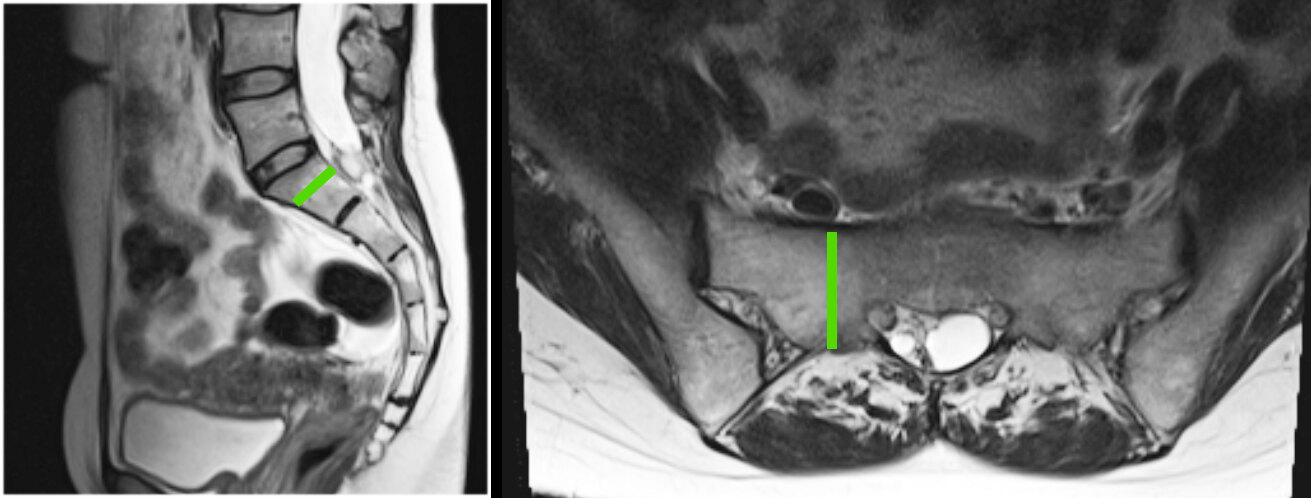
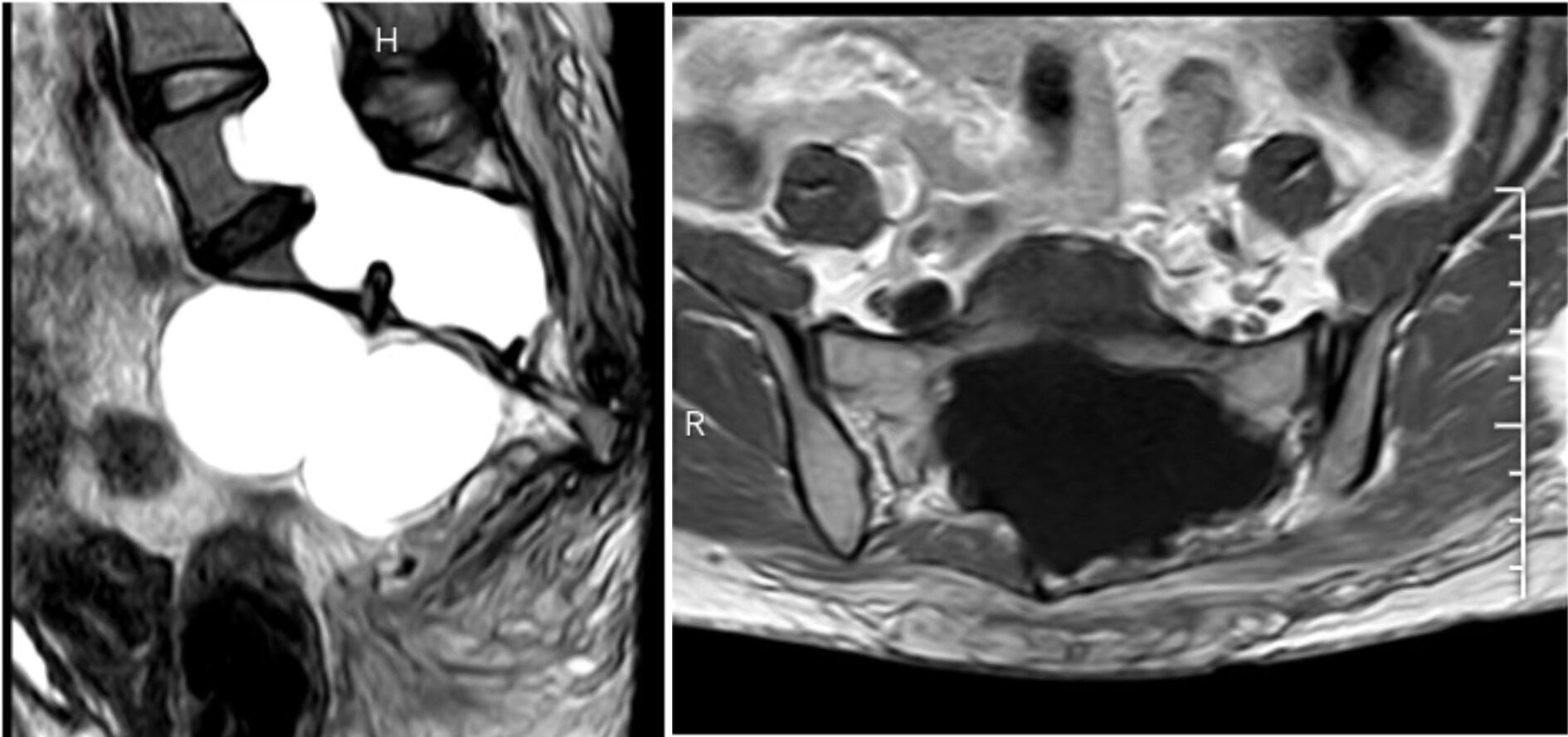
Large sacral cysts lead to chronic erosion of the sacrum. Dr. Xuesheng Zheng’s team has always prioritized the protection of the sacral bone and the repair of the posterior wall of the sacral canal during surgical procedures. This is essential to prevent the protrusion of the sacral canal’s contents. For a deeper understanding, please refer to our previous article titled:
“Minimally Invasive Surgical Concept for Sacral Canal Cysts: Maximizing Bone Protection.”
“This comprehensive guide covers all aspects of minimally invasive surgery for sacral cysts, including detailed explanations with pictures and text. It is highly recommended for those interested in this topic.”
“A case study on minimally invasive surgery for multiple giant sacral cysts.”
“A case of giant Tarlov cyst by Dr. Zheng’s team with a mere 4.5cm incision.”
Today, we will delve into the significance of repairing the posterior wall of the sacral canal from the perspective of the sacral vertebrae’s weight-bearing capacity and stability.
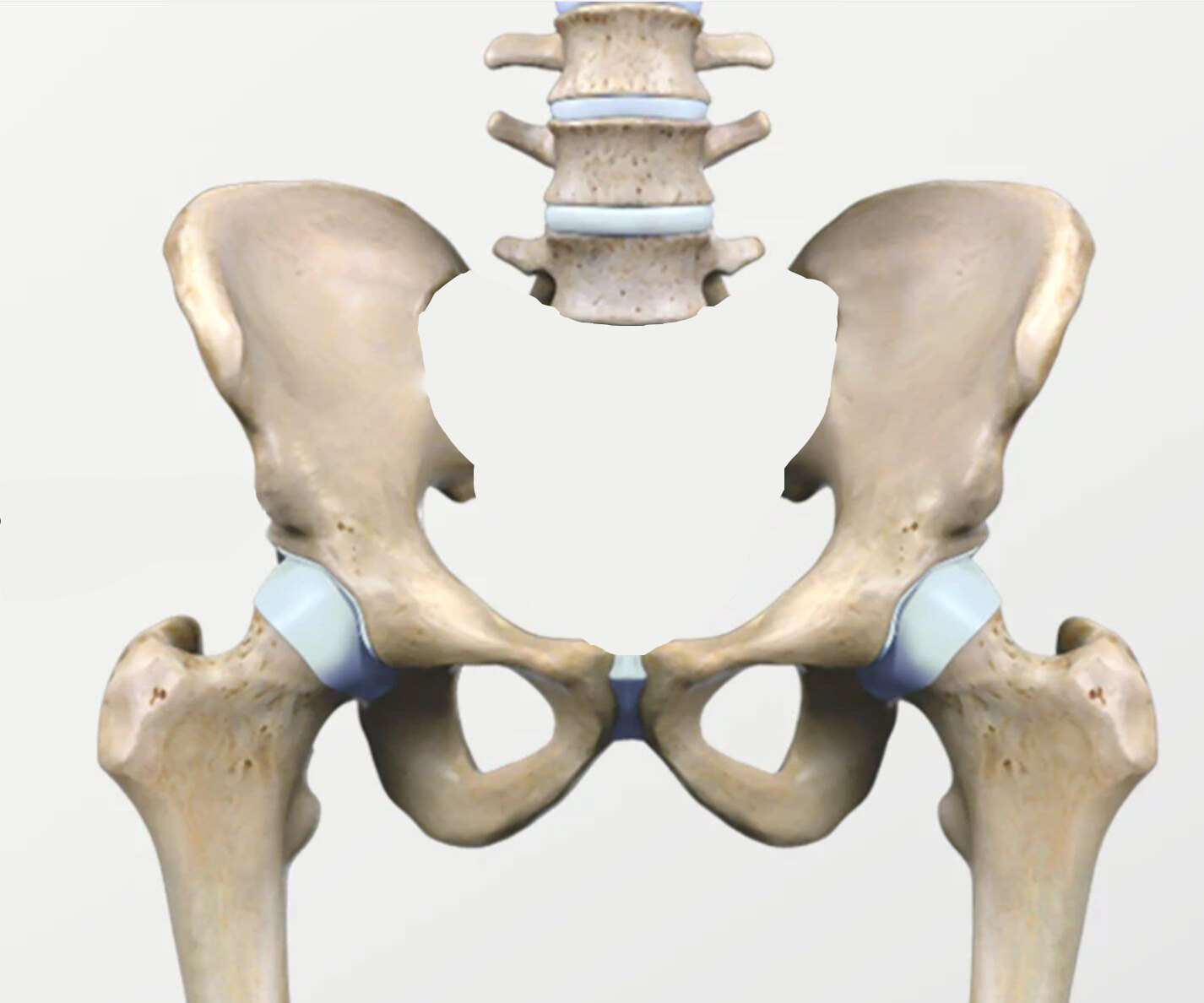
Consider a patient weighing 60 kilograms. The weight above the lumbar spine, approximately 40 kilograms, is transmitted through the lumbar spine to the sacral vertebrae (primarily sacral 1-2), then through the sacroiliac joint to the pelvis, and finally through the hip joint to the lower limbs.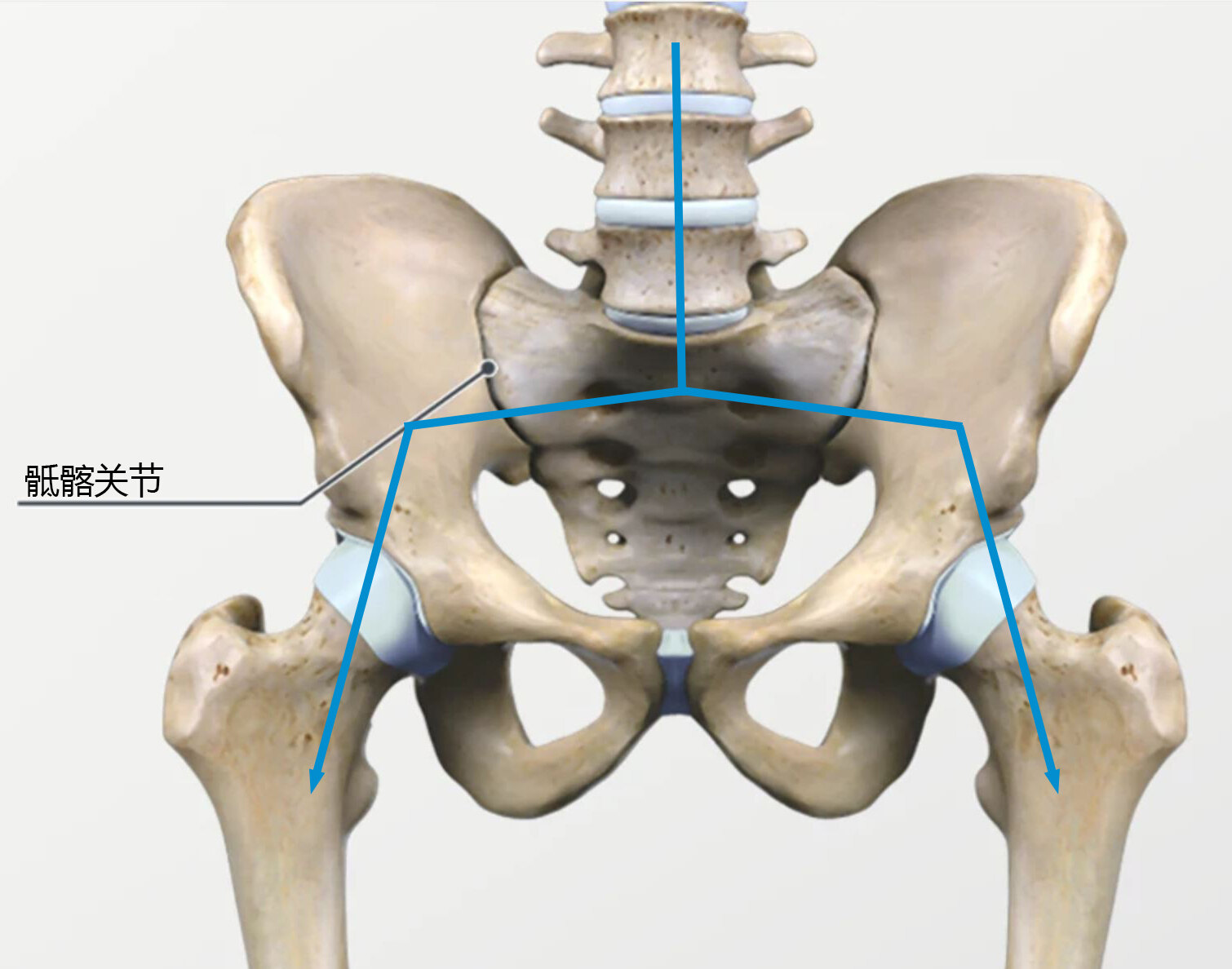

In summary:
Sacral canal cyst surgery should prioritize the use of small bone windows to minimize bone structure disruption.
Accurate location of leakage is essential to avoid the need for expanding the bone window.
The bone defect in the posterior wall of the sacral canal caused by the lesion itself should be fully utilized, with slight expansion to form a small bone window.
After successful closure, titanium plates should be used to repair the bone defects in the posterior wall of the sacral canal, restoring the sacral canal’s basic shape and maintaining the stability and weight-bearing capacity of the sacral vertebrae. The importance of posterior wall repair increases with the size of the sacral cyst.